
Expert Forum
Painful Blisters
Herpes Zoster in Traditional European Naturopathy
For those in a hurry
Herpes zoster is caused by a reactivation of the varicella-zoster virus in a weakened immune system. In addition to anti-viral therapy, naturopathy focuses on strengthening the lymphatic system, constitution and milieu. The goal is to accompany acute processes and prevent post-herpetic neuralgia.
Herpes zoster is more than just a painful rash: the resurgence of the varicella-zoster virus can cause long-lasting nerve pain. Friedemann Garvelmann explains the naturopathic connections and therapy options in his article.

Conventional medicine sees shingles as the later secondary disease of a primary varicella disease (chickenpox), which usually takes place in childhood. It is triggered by the varicella-zoster virus (VZV), one of the eight herpes viruses that are pathogenic to humans and vertebrates. According to the RKI*, antibodies against VZV can be detected in 95% of all people. This means that almost everyone has contact with this virus in their lives, usually in childhood, when it manifests itself as chickenpox disease (provided that the organism has the disposition to do so). However, the formation of anti-bodies can also take place without symptoms in a ‘silent release’ and, in the optimal case, protects the affected person from a second disease for the rest of his or her life. Every self-sufficiently thinking person must find an independent assessment of whether a disease such as chickenpox, which is harmless to a constitutionally stable child, really needs the prevention of comprehensive vaccinations. Even though it is known that immunity induced by vaccination is significantly inferior to immunity acquired with the disease and is also limited in time.
After the initial infection with VZV, the viruses are not eliminated from the body, but rather remain in spinal ganglia or are permanently kept in check by an intact functioning immune system (pathogen persistence). A short preliminary remark: As soon as terms such as virus, infection, antibody or immune system appear, we have left the territory of naturopathy and find ourselves mentally in the infectious diseases of conventional medicine – no matter what means and methods we use to treat them.
Weakening of the lymphatic defense can lead to the reactivation of the viruses, which are then manifested as a secondary disease in the form of acute zosters. Herpes zoster can therefore not be transmitted directly, but rather always via a varicella primary disease.
This confirms Claude Bernard’s finding, which is very important in naturopathy: “The pathogen is nothing, the milieu is everything” – whereby the term milieu here stands for the stability or the instability of the functionality, especially of the lymphatic system. The focus of consideration (also in therapy) should therefore not be on the virus, but rather on the constitutional state of the host organism. This raises the question of the background to constitutional weakening, which of course must always be answered individually. Here are some common aspects – without claiming to be exhaustive:
The statement that immunity to VZV decreases over time is only plausible if immunity is not naturally boosted by contact with VZV from time to time.
The statement that immunity to VZV decreases over time is only plausible if immunity is not naturally boosted by contact with VZV from time to time. In a society in which chickenpox is accepted as a common (rather even necessary) event in childhood and therefore VZV is always in circulation, such a booster is almost inevitable in adults. This implies the heretical question of whether it is not precisely the reduction of chickenpox by vaccinating children that prevents the immunity of adults from being refreshed? Although the vaccination industry tries to compensate for this by vaccinating adults (> 60 years of age), the significant increase in severe zoster cases shows the unconvincing efficiency of this strategy.
After five years, it can be assumed that herpes zoster is a typical and frequent consequence of the gene-altering modRNA injections against Corona. In this regard, the research results of independent scientists around the world can be summarized in short form as follows: The modRNA injections cause serious pathological, often autoaggressive modifications of the immune reactions due to the programmed production of the spike proteins, which are largely irreversible according to current knowledge. One of the very common and rapidly occurring consequences, especially after repeated injections, is the significant increase in severe zoster cases, often combined with other manifestations of Post-Vac Syndromes. The author of this paper has become aware of countless zoster cases in his own environment and in the course of his seminar activities, some between the ages of 20 and 30. This should be particularly alarming, because the occurrence of zoster at such a young age was already considered an alarm signal for serious immune deficiencies long before Corona.
The increasing prescription of immunosuppressive drugs for many different diseases, with corticosteroids still being among the milder ones, logically also weakens the immune system’s ability to keep VZV inactive.
Symptoms and Course
The reactivation of VZV causes acute inflammation of the affected spinal nerve. The strictly one-sided course in one segment (monosegmental) is typical, but it is not uncommon for inflammation of several adjacent nerves of the segments above or below it. In the case presented at the end of this paper, 5 segments were affected. The distinguishing feature is the striped or belt-shaped reddening of the dermatome belonging to the affected spinal nerve with initially serous filled vesicles, which subsequently become pustular, open and then heal encrusted. The event is accompanied by pulling, burning and also neuralgic shooting pain, often with very strong intensity. The first symptoms on the skin are itching and paresthesia, often even before the first visible inflammatory reactions. Particularly striking is the occurrence of seemingly unfounded general fatigue, exhaustion and depressive moods, already 1-2 weeks before the appearance of the typical symptoms of zoster. This clearly shows that this is not a purely local, but rather a systemic disease process. But more on that later.
If the eye or ear are affected, intensive antiviral and anti-inflammatory therapy is usually necessary.
Decisive for assessment of the disease risk, the prognosis, and groundbreaking for therapy, is the localization of the affected segments. If the skin symptoms occur on the torso or leg, the disease can usually be treated quickly and efficiently with pure naturopathy. However, if the eye or ear are affected, intensive antiviral and anti-inflammatory therapy is usually necessary to prevent consequential damage to the sensory organs. The same applies to zoster in the area of the genital organs.
At this point, the biological significance of acute inflammation (unfortunately far too often ignored) should be recalled: In contrast to chronic inflammation (silent inflammation), the process of acute inflammation is the most efficient, evolutionarily acquired defending and overcoming mechanism, which is stereotypically set in motion by pathogenic stimuli. Acute inflammation proceeds with the known inflammatory phases and serves the goal not only of achieving the much-cited restitutio ad integrum, but also of overcoming the triggering stimulus, which should also be understood as the deletion of pathogenic information. This results in positive learning processes that can be used to overcome similar disease triggers later on. From this point of view, immunity is certainly not only based on the ability to form corresponding antibodies, but is rather also an informational, epigenetically based process.
The Pathophysiology From A Broader Perspective
“The blister rash is caused by the spread of inflammation from a nerve (…) on the surrounding dermatome“. This explanation, which is basically found in most textbooks, sounds plausible at first glance and is therefore usually not questioned further. However, the humoral medical view of TEN** does recognize some inconsistencies that are very valuable for understanding the systemic pathophysiology of herpes zoster, its symptoms, its course and its dreaded complications (post-herpetic neuralgia, or zoster residual neuralgia).
For example, it is not a self-evident fact that the skin reacts to inflammation of a peripheral nerve. In the case of vertebral irritation syndromes, for example, this is usually not the case either.
Since all nerve tissues have an extremely weak ability to defend themselves against infectious agents, consensual support from more immunocompetent tissues is necessary to overcome the viral stimulus. In the case of herpes zoster, this is the skin, also of ectodermal origin. To put it very figuratively, the nerve asks for the help of the skin in overcoming the pathogenic factors. Such a displacement of a disease process is called vicariation in the TEN, a pathophysiological mechanism that is often observed in very different diseases. Although it primarily takes place as a vicariation from the skin to mucous membranes (or vice versa), it can also take place reciprocally between almost all other tissues.
If you look at it on the basis of Humoral Medicine pathophysiology, VZV acts as a sharpness with a choleric quality (hot and dry). Above all, the hot quality of the sharpness is recognizable in all aspects of the disease: rapid onset, acute inflammation, severe pain, burning, cutting and neuralgic. The dry quality is responsible for exhaustion (energy deficiency syndrome).
In naturopathy, exudative processes of the skin type are generally seen as a replacement excretory mechanism for pathological fluids that cannot be eliminated by the entire organism via the physiological excretory organs. Of course, this also applies to the typical skin lesions in zoster. They represent the natural, very efficient excretory valve that helps the patient to excrete the yellow-bile sharpness. In combination with acute inflammation, vicariation and dermal replacement excretion are extremely important mechanisms of the organism’s self-healing strategy. If the physiological sewage flow for the removal and discharge of the sharpness is deficient and in addition the described dermal substitute excretions are too inactive or they are pharmaceutically suppressed, the choleric sharpness cannot be excreted to the necessary extent and become a chronic burden with corresponding yellow-bile consequences.
The persistent sharpness becomes a permanent trigger of the nerve, which responds to it with pain.
Post-Herpetic Neuralgia
This mechanism is the pathophysiological background for many chronic pain conditions that persist after the skin symptoms of zoster have healed, often for many months, sometimes years. The persistent sharpness becomes a permanent trigger of the nerve, which responds with pain. The result is chronic post-herpetic neuralgia, which can be so unbearable for the affected person that he or she develops suicidal thoughts. Practical experience shows that these chronic pain conditions are often much more resistant to therapy than the acute phase.
Many cases of post-herpetic neuralgia could be avoided.
However, many cases of post-herpetic neuralgia could be avoided by observing, respecting and sensibly supporting the pathophysiology of substitute excretion described above. The logical consequence for therapy of the acute phase is therefore that the acute inflammatory overcoming processes, including dermal substitution excretion, must not be suppressed. But that’s exactly what all anti-inflammatory and antiviral drugs do.
According to the author’s experience, post-herpetic neuralgia is extremely rare in patients who have been treated according to naturopathic principles. This implies the question of whether [or not] it is really in the interest of the affected patient during an acute phase with the most severe chronic pain, to buy a few shortened days by means of acyclovir and the like.
Therapy Suggestions For the Acute Phase:
Therapy goals here are:
- stabilization of energy reserves as a prerequisite for the successful overcoming and healing processes
- Stimulation of the defense dynamic: Only functions if the necessary physiological heat is available (see first point)
- Support of the lymphatic system, both in the area of drainage and immune functions
- Stimulation of the elimination of yellow-bile sharpness via the physiological excretory organs in order to relieve the skin
- Pain relief and nerve regeneration
An individual definition of the therapy goals is a prerequisite for the methodical implementation.
As with any therapy concept, the individual definition of the therapy goals is a prerequisite for the methodical implementation. That means, the question of which remedies and methods can be used to achieve these therapeutic goals most efficiently. The treatment options listed here are based on the drug therapy of traditional naturopathy. Depending on the therapist’s way of working, they can be used as individual or complex remedies or in individual formulations.
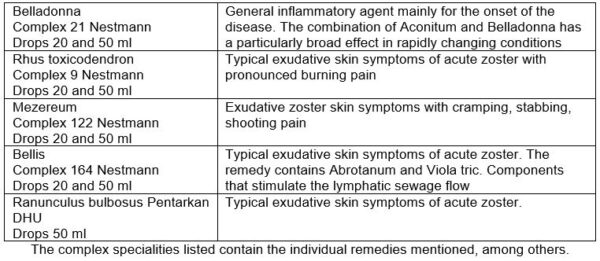
The following individual remedies represent the bullous and pustular skin symptoms typical of the acute phase of herpes zoster:
- Clematis D6
- Mezereum D6
- Ranunculus bulbosus D6
- Rhus toxicodendron D6 (The potentiation level is of course completely variable, but the D6 has proven itself universally.)
St. John’s wort is at the top of the list when it comes to pain relief.
The following have proven to be painkillers:
Hypericum D4
St. John’s wort is at the top of the list of pain relief in zoster in all phases. In some patients, it is the only remedy that efficiently relieves the pain (also in comparison with ibuprofen, paracetamol, Novalgin). The prerequisite is that the patient does not take it according to a rigid dosage rule, but as often as he needs it, possibly 10 drops every quarter of an hour. It is therefore advisable to prescribe Hypericum D4 dil. not (only) in formulations for complexes, but also individually in a 100 ml bottle.
Hypericum is also an excellent stimulant for the regeneration of all nerve tissues, which is an important aspect in post-herpetic neuralgia.
Belladonna D6
Severe, even neuralgic pain on the basis of acute, even febrile, inflammation. Heat is in the periphery with sweat. The patient is very restless, to the point of frenzy.
Aconite D6
Severe, even neuralgic pain on the basis of acute, even febrile inflammation. Heat still inside, periphery is cold, without sweat. Patient is anxious and apathetic.
Colocynthis D6
Cramping pain and neuralgia, especially in people with a chologenic (biliary) constitution and spasmophilic diathesis.
Hyoscyamus D6
An important remedy for normalizing the exaggerated sensitivity and irritability of the nervous system.
The complex specialties listed below include, among others, the individual remedies mentioned above. It goes without saying that you don’t use them all together, but selectively use one or two of them, as suitable as possible to the patient’s disease situation.
Stimulation of immune functions:
- Geranium robertianum ø
- Echinacea purpurea ø or as a speciality
- Vincetoxicum ø or D2 lymphatic remedy
- Scrophularia nodosa ø
- Viola tricolor ø or Violae tricol. Hb. as Infus
- Calendula officinalis ø or Calendulae Flor. as an infus
Other supplementary remedies that stimulate physiological heat as well as promote elimination on yellow-bile sharpness:
- Taraxacum offic. ø
- Fumaria ø
From these remedies, two individual prescription suggestions for drug therapy in the zoster acute phase:
- Bellis Complex Nestmann 50 ml
- Scrophularia ø 20 ml
- Fumaria ø 30 ml
- Geranium robert. ø 50 ml
M. f. dil.
DS: 10 drops every 2 hours
also: Hypericum D4 100 ml
DS: 10 drops as often as desired for pain relief
- Ranunculus Pentarkan 50 ml
- Vincetoxium D2 20 ml
- Viola tricol ø 30 ml
- Taraxacum ø 50 ml
M. f. dil.
DS: 10 drops every 2 hours
also: Hypericum D4 100 ml
DS: 10 drops as often as desired for pain relief
The intake of neurotropic vitamins can dampen overstimulation of the affected nerves.
Vitamin B Complex
The intake of neurotropic vitamins can dampen the overstimulation of the affected nerves. For example: Vitamin B Loges complete capsules, Vitamin B Complex forte (Hevert).
To compensate for the poor absorption of B vitamins in the intestine, a corresponding vitamin B complex can also be administered once or twice by injection at the beginning of treatment, also as a further addition to the autologous blood therapy described below.
The mixed injection is administered intragluteally twice a week.
Autologous Blood Therapy
One of the most efficient methods for modifying and stabilizing immune functions is treatment with i.m.-injected autologous blood. In acute zoster, the following injection schedule has proven effective in the author’s practice:
- Injection: 0.5 ml venous blood
- Injection: 1.0 ml venous blood
- Injection: 1.5 ml venous blood
- Injection: 2.0 ml venous blood
Mix in each: 1 Amp. Infi-Colocynthis injection (Infirmarius) and 1 Amp. Engystol (Heel)
This mixed injection is administered intragluteally twice a week, which is possible without any problems with the maximum total amount of injection fluid and almost painlessly with slow injection. A maximum of ten injections in total in a series, which can be repeated after three months if necessary. With regard to autologous blood therapy, the local legal regulations must of course be observed.
Notes On External Therapy
The skin area affected by acute herpes zoster is often so sensitive to pain that even the application of an ointment or lotion is unbearable for the patient. In these cases, virtually no external support is possible, at least temporarily. Only the application of a powder is usually tolerated. However, the powder used should not contain zinc oxide (or other zinc compounds), as these can block the described sharpness elimination through the skin. The Wecesin powder (Weleda) can be used, which supports healing with plant and mineral components.
If the skin sensitivity has subsided to such an extent that it is possible to apply a lotion, the Galium lotion from Amidor Naturkosmetik, which is formulated with extracts of Echtem Labkraut (Galium verum) as well as Natr. Phos. D6 and Natr. sulf. D6 reduces the sharpening effect and supports the nurturing healing without restricting the necessary excretion processes.

Figure 1 to 3: Patient with left-sided lumbosacral herpes zoster up to the lower leg
Therapy for Pain After the Acute Phase
For treatment after the acute phase has already expired, the therapeutic approaches must be set differently. The stimulation of lymphatic immune functions and skin symptoms are no longer the focus. To this end, the analgesic regulation of nerve excitability and the elimination and detoxification of choleric sharpness become the focus, whereby drainage methods can now also be used, which are often not possible in the acute phase for reasons of pain. Summarized therapy goals are now:
- Stabilization of the general energetic situation – as a prerequisite for all further therapeutic approaches
- Stimulation of the elimination and drainage of yellow-bile sharpness
- Pain relief (based on 2.)
- Stimulation of nerve regeneration and stabilization of its excitability
The constitutional situation of the patient plays a major role here, because the tendency to chronification, non-healing and excessive irritability of the affected peripheral nerve (often neurasthenia) is to a large extent constitutional.
Colleagues who have mastered iris diagnosis-based constitutional medicine have a clear advantage here, because only in this way can the underlying systemic pathophysiology be precisely recorded and the therapy concept focused accordingly.
A good start to therapy is the one-time administration of five globuli of Herpes zoster nosode 200 C. Figuratively speaking, this nosode reminds the healing systems in a purely informational form to take care of the even still unresolved topic of herpes zoster. In this way, the effect of this nosode is often experienced as a specific activator of blocked self-healing mechanisms, which is a prerequisite for the efficiency of other therapeutic approaches. A second dose of Herpes Zoster Nosode can be given after about four weeks if necessary. Experience has shown that more frequent and further doses are not necessary, but they are quite possible.
Drug Therapy:
This consists of:
- Mezereum Capsules Nestmann 50 ml
- Juglans ø 20 ml
- Fumaria ø 30 ml
M. f. dil.
DS: 3 x daily 20 drops before eating
in addition: Hypericum D4 100 ml
DS: 10 drops as often as desired
For some patients with restlessness and anxiety, or the diverse symptoms of vegetative dysregulation, it makes sense to focus on the general calming and strengthening of the nervous system:
- Sabadilla Capsules Nestmann 50 ml
- Scrophularia ø 20 ml
- Fumaria ø 50 ml
- Rhodiola rosea ø 30 ml
M. f. dil.
DS: 3 x daily 20 drops before eating
in addition: Hypericum D4 100 ml
DS: 10 drops as often as desired
The paravertebral skin zone above the spinal nerves is treated.
Elimination and Drainage Procedures
Due to the skin symptoms and the severe pain, elimination and drainage [detoxification] procedures applied to the skin are usually not possible or only possible to a very limited extent in the acute phase of herpes zoster. In post-herpetic pain on the other hand, they are extremely helpful, often the ‘game changers’. The principle of action of all detoxification procedures in which the skin is opened imitates the cutaneous excretion processes for sharpness, which take place spontaneously in the form of blisters and pustules in the acute zoster phase. This also offers therapeutic possibilities in subsequent phases to drain the yellow-bile sharpness responsible for the persistent pain via the corresponding reflex zones of the skin. The following methods can be used: Cantharidin blister, leeches, bloody cupping. In each case, above the paravertebral skin zone or the spinal nerve(s) in which the pain manifests itself is treated, on one side of the pain, about a hand’s breadth. The prerequisite is that the skin in this area is intact and not excessively sensitive to pain. In these zones, local muscle tension (myogelosis), heat zones, redness and/or edematous cushions in the skin are often found in a palpatory manner (indication of stagnation in the lymphatic sewage flow). Occasionally, there is also increased sensitivity to touch or palpation. Based on these findings, it is possible in many cases to identify the individual trigger points or zones through inspection and palpation in dialogue with the patient. The more precisely the treatment is carried out on the trigger points, the more pronounced the effect. Otherwise, of course, all application criteria apply that must be observed for the respective method anyway. Unfortunately, these methods can only be used to a limited extent in the area of the cervical spine and at the back of the head.
The contents are drained by opening the blister.
Cantharidin Blister
In the indicated skin zone of the affected segment, a Cantharidin blister is created by a blistering plaster with a diameter of approx. 4 cm. After that, the contents are drained by opening the blister. If the sensitivity to pain allows, the skin over the blister should be completely removed, this further enhances the effect. Wound care is carried out as described in the previously mentioned textbook. The placement of a Cantharidin blister can be repeated after about 4 weeks – but this will not be necessary in most cases.
The placement of Cantharidin blisters has its main effect on the lymphatic level – which is important for the selection of methods according to the criteria of Humoral Medicine.
The postoperative bleeding should be able to drain unhindered during leech therapy
Leeches
In the indicated skin zone of the affected segment, two to four leeches are placed according to the usual rules of leech therapy. With regard to localization and/or appointed time, care must be taken to ensure that the postoperative bleeding can drain unhindered. Leech therapy can also be repeated after about 4 weeks if necessary.
The placement of leeches has its main effect at the blood level – which is important for the selection of methods according to the criteria of Humoral Medicine.
Dry cupping is usually not useful.
Bloody Cupping
In the indicated skin zone of the affected segment, one or two bloody cupping glasses are placed according to the usual rules of cupping therapy. That means, the skin under the cupping glass is perforated 10-12 times with a blood lancet. This procedure can be used weekly if necessary. Dry cupping is usually not useful in this situation, because it can increase the heat principle and flow of fluids – and thus the pain – through its toning effect. Unless the paravertebral skin and tissue findings indicate dry cupping.
Baunscheidt Procedure
This is a process with histamine-containing oil. It should be noted that this is a drainage method that acts at the lymphatic level, the effect of which depends heavily on the constitutional resilience of the lymphatic system. This everyday method can be used daily, several days in a row.
Neural Therapy
Using a mixed injection of procaine and Infi-Colocynthis injection (Infirmarius), intracutaneously wheal the skin zones described in the elimination and drainage procedures. If subcutaneous or muscular trigger points are present, this mixture can also be injected directly into them.
Case Study
The 87-year-old patient presented here had herpes zoster, whose skin symptoms spread on the left side from the lumbosacral junction to the lower leg. The segments L1 to L5 were affected (see figures).
As expected, the pain was very severe. Ibuprofen and Novalgin did not show any significant effect, but taken with Hypericum D4 in the manner described above, they were well tolerated. Otherwise, the treatment was carried out as described above purely naturopathically (without viral agent), including autologous blood i.m.
Result: After 6 weeks, the skin had healed without scarring and the patient was permanently pain-free.

An Exclusive Translated Article for P2P Supporters
From the Monthly Publications of P2P
Published April 2026
From an article in Naturheilpraxis, Volume 79, March 2026
Translation & redaction by: Carolyn L. Winsor, P2P Consulting
© Copyright 2026, Naturheilpraxis, Friedemann Gravelmann, Germany
AI Digital and online translation assistance utilized.

Footnotes:
* RKI = Robert Koch Institute, Germany
** TEN = Toxic epidermal necrolysis
Literature
- Jajou R, et al. GP Consultations for Herpes Zoster After COVID-19 Vaccination: A Self-Controlled Cohort Study Based on Electronic Health Record Data from the Netherlands, Springer Nature 2025.
- Garvelmann , Müller. Ab- und Ausleitung in der TEN/TEM, Bacopa
- Epoch Times: Studien zeigen: Covid-19-Impfung reaktiviert Windpockenvirus, n.rpv.media/8xu.
")
