
Abstract
At the beginning of the COVID-19 pandemic, the acute infection was the focus of interest, but since then the perspective has changed. After the infection, impairments may persist in those affected, at both the physical as well as the mental level – the so-called “Long-Covid Syndrome” or “Post-Covid Syndrome”. The healthcare system is doing research on causes and treatment options. In practice it has been shown that previously well-established naturopathic procedures make a positive contribution to the therapy of patients with Long-Covid. Especially the combination of orthodox medicine and naturopathy in the sense of an integrative therapeutic approach can offer a broad spectrum of targeted treatment measures. These measures could do justice to the extent of the consequences of COVID-19 infection with its range of symptoms which patients sometime perceive as very burdensome.
Keywords: Long-Covid, Post-Covid, Krankenhaus für Naturheilweisen (Clinic for Internal Medicine, Naturopathy and Homeopathy), KfN, Naturopathy

Translator Note: Krankenhaus für Naturheilweisen (KfN) has been translated in at least three ways in the literature as The Hospital for Naturopathic Medicine, for Natural Medicine and for Natural Healing. Located in Munich, it is one of the leading complementary medicine clinics in Germany. For more than 100 years, they have been integrating recognized procedures from complementary medicine such as naturopathy and classic homeopathy, into scientifically based conventional medical treatment concepts. For the purposes of this article I will remain with the more colloquially and commonly used translation of “Naturopathic”, although “natural medicine” would likely be more applicable in light of the many different complementary therapies they utilize. You can visit their website here: https://www.krankenhaus-naturheilweisen.de/ (and Mr. Google will happily translate for you).
The corona pandemic which has meanwhile spread to all corners of our globe, has us more than ever in its grasp. The long-term consequences of an acute COVID-19 infection now known as Long-Covid and/or Post-Covid Syndrome, seems to take on an enormous importance. The significance can only vaguely be foreseen and seems to convey a quiet feeling of powerlessness considering the many people affected, since the disease leaves traces with severe but already with mild courses. Quality of life and everyday life are suddenly enormously limited which also has considerable consequences for the social environment(1).
S1 Guideline
So far, neither the exact cause nor a causal therapy is known. Science is researching worldwide under high pressure. Not only frequency, causes and symptoms are the subject of current research. Knowledge about well-founded and practicable methods for diagnostic and therapeutic options must be gained. Thus in July 2021 the first S1 Guideline for Post-Covid/Long-Covid(1) was drawn up for medical professionals by 16 medical societies, led by the Society for Pulmonology and Respiratory Medicine (DGP). Due to a great deal of uncertainty among patients, there was the first patient guideline for those affected written by C. Gogoll as a result.
Long-Covid is designated according to the S1 Guideline for Post-Covid/Long-Covid as persistent symptoms of a COVID-19 infection from the onset of infection beyond 4 weeks or the appearance of new symptoms after the end of the acute phase. In this case it concerns symptoms which are understood as the result of a COVID-19 infection or have led to a new illness. It can also be a “worsening of a pre-existing underlying disease”. If the symptoms persist for more than 12 weeks, it speaks about Post-Covid(1). According to the supplementary definition of the WHO however, these complaints must also persist for at least 2 months(2). Thus Long-Covid includes the Post-Covid syndrome.
According to the S1 Guideline for Post-Covid/Long-Covid of July 2021, to date the pathomechanism of Long-Covid (LC) could not be fully clarified(1). According to Kopczulla et al. a viral persistence, damage to the tissues themselves in the area of the endothelium, a disturbed micro-vascularization as well as effects of a (hyper)inflammation among others could be involved causally(1).
Prevalence and Incidence
Currently there are still many uncertainties existing in relation to prevalence and incidence. It is described in the broad literature that LC probably pertains to between 10% and 20% of all patients after a SARS-CoV-2 infection. The WHO also assumes this prevalence(2) (3). According to the S1 Guideline for Post-Covid/Long-Covid of July 2021 there probably exists a frequency of 15% according to the population examined(1). Possible predictors of LC are primarily female gender and the presence of more than 5 symptoms during acute illness, as well as a higher severity of COVID-19 infection(2). So far it has also become known that the development of LC is favored by pre-existing conditions as well as by a severe course of COVID-19 infection. Young and middle-aged adults are more likely to be affected.
The symptoms of LC are very diverse, but can usually also be completely non-specific. Patients often suffer from pronounced tiredness and exhaustion as well as limited resilience. In most patients this comes to the foreground of the symptoms, followed by persistent breathing difficulties as well as smell and taste disorders. Additionally the current relevant literature also describes cognitive complaints like concentration and memory problems, muscles weakness, muscle pains, headaches, joint pains, cough and sleep disturbances, but also depressive moods and anxiety symptoms(1) (2).
These complaints can already occur in less symptomatic courses and especially in young people, continue for many months and also become chronic. The good news is however that the symptoms usually decrease over time(2) (3).
Nevertheless, organic sequelae are already described in the context of low symptomatic disease courses, and these are known to occur more frequently after severe courses. Scientists within the framework of a large scale study at the University Medical Center Hamburg-Eppendorf (UKE) under the direction of R. Twerenbold have already produced the proof that as a result of mild/moderate courses of COVID-19 infection not only the functions of the heart, lungs and kidneys are impaired in the medium term, but there also existed an increased prevalence of deep leg vein thrombosis(3). They recommend after half a year or at the latest after 9 months systematic screening examinations, e.g. NT-proBNP and GFR and if necessary further examinations in the sense of echocardiography or body plethysmography in the case of persistent respiratory complaints as well as the implementation of an ultrasound leg vein doppler in the slightest suspicion of deep leg vein thrombosis(3).
Peterson et al. report that more than 10 clinics at the University Medical Center Hamburg-Eppendorf were involved in the study. Another very large-scale study has already started with the goal of identifying risk factors for cardiovascular disease(3).
There is a need for multidisciplinary cooperation. Other causes of the complaints must be excluded, because according to Pink and Welte Long-Covid is still a diagnosis by exclusion(2). On the other hand an adequate treatment must be initiated promptly in sequelae to the end organs, because even initially severe courses are accompanied with an increased risk of cardiovascular complications(1) (2).
On the other side according to the Robert Koch Institute (as of 11.07.2022) previously existing underlying diseases also seem to increase the risk for Long-Covid, especially in the presence of a high viral load, the presence of specific autoantibodies, the evidence of previous EBV infection and also with diabetes mellitus, if this is pre-known. In this context it is also pointed out, among other things, to the increased risk of LC with people affiliated in the health professions.
Symptomatology
Most patients with LC complain about tiredness, exhaustion and limited resilience. The symptoms are referred to as fatigue and are very similar to those of chronic fatigue syndrome (ME/CFS, myalgic encephalomyelitis), which can be the result of infectious diseases such as EBV or borreliosis, but also appears – rather rarely – idiopathic(1).
Patients are massively limited in their performance capacity even in light everyday activity and quickly exhausted. Any form of rest does not change this, the patients may need perhaps days to restore their original state. It the load limit is exceeded, post-exertional malaise (PEM) occurs. Due to fatigue however, the quality of life is massively limited in all areas, which particularly affects the working environment and social contacts, especially when patients do not seem ill and feel misunderstood.
Very often cough and dyspnea are as component of the symptomatology of LC, additionally there may also be a feeling of thoracic pressure. Fortunately dyspnea improves in most patients during the illness course(4). However according to a study by Sommer and Schmeck from the Pulmonological Institute of the University Hospital Giessen and Marburg, interstitial changes in X-ray findings, restrictive changes in lung function and restrictions in diffusion capacity often appeared after a severe COVID-19 infection. The authors concluded that there is still no clarity about what relevance these findings bring with them, or what role is played by other factors, e.g. in the context of a hospitalization or also pre-existing illnesses(4). The authors further reported that “Asthma has been identified as a risk factor for persistent discomfort after COVID-19.” What relevance a pulmovascular involvement has in Long-Covid has also not yet been clarified. Sommer and Schmeck conclude that “due to a lack of studies, there are still no evidence-based guidelines for the diagnosis or treatment of pulmonary manifestations with Long-Covid Syndrome”. In their work from July 2022 they provide a helpful overview of the procedure for diagnostic as well as therapeutic approaches with regard to the respective symptoms, whereby the S1 Guideline on Post-Covid/Long-Covid from July 2021 still represents the previous treatment basis(4).
Hennings, et al. found significant changes in the respiratory muscles in their work 5 months after infection even in non-hospitalized patients(5). Women were predominantly affected. The authors demand systematic diagnostic check-ups in symptomatic patients in the context of Long-Covid(5). COVID-19 can also clearly leave its traces on the cardiovascular system, often through autonomic dysregulation accompanied by tachycardia or blood pressure fluctuations. However especially after severe courses of COVID-19 the risk of complications such as myocardial infarction, apoplexy and thrombosis is increased(1).
Neurological symptoms as well as smell and taste disorders are widespread, which often lead to an unexpected severe reduction in quality of life. Ott reports from a recent study from Singapore by Tan et al. that the senses of taste and smell can be changed in the long term in a relatively high number of patients, mainly women(6) (7) (13).
Depressive moods also often occur in the context of Long-Covid, but this must however be clearly distinguished from depression in the context of the pandemic. A questionnaire can be helpful here as a first screening too, e.g. PHQ-9.
Diagnosis
Family doctors are often the first contact for making a diagnosis because patients often come to the family doctor’s office with a series of symptoms that can be associated with the original infection. Specific laboratory values and examination methods for classification do not yet exist, however LC cannot be excluded even by imperceptible laboratory values(1). Functional limitations must therefore be objectified. Only after a thorough anamneses as well as a primarily medical physical examination with observance of the “Red Flags”, exclusion of avoidably dangerous courses as well as careful differential diagnosis can a primarily LC assessment be raised. If this can be classified in the definition of a LC, e.g. according to the S1 Guideline of July 2021, a diagnosis can be made.
Networking with a wide variety of professional disciplines, a multidisciplinary approach to the exclusion of possible differential diagnoses, securing the diagnosis(es) and the timely initiation of further therapy options are always crucial.
Therapy
According to the recommendations of the S1 Guideline on Post-Covid/Long-Covid from July 2021, the therapy for LC basically occurs purely symptomatically(1). At the same time patients feel taken seriously and psychosocial support can also be offered(1). The possibility and ability of rehabilitation must be thoroughly examined.
The connection to self-help groups is a crucial approach for the patient. In the case of high psychological strain and unclear findings they can also be conveyed to special outpatient clinics which meanwhile have also been established at some medical centers all over Germany.
Since subclinical multiorgan involvement in lungs, heart, kidneys and vascular system can persist months after infection in patients with mild courses who have obviously recovered, Petersen et al. recommend within that context a “comprehensive multi-organ assessment” of systematic screening tests within 6-9 months after mild to moderate SARS-CoV-2 infection(3).
The best protection against Long-Covid is probably still the complete vaccination against SARS-CoV-2 including compliance with hygiene measures (AHA + L) but especially the correct wearing of FFP2 masks or mouth-nose protection in accordance with the current recommendations of the Ministry of Health and RKI.
In their work on topic of vaccination against SARS-CoV-2 in patients with Long-Covid, Bauernfeind and Schmidt found out that just with breakthrough infections (fully) vaccinated people presumably have a lower risk of falling ill with Long-Covid. The authors further explain with regard to vaccination as a therapeutic option: “An additional therapeutic benefit in existing Long-Covid is still unclear”(8). Vaccinations and hygiene measures thus continue to play a major role in limiting infection with COVID-19 and thus Long-Covid.
In Practice
The family doctor is usually the first point of contact for those affected and coordinates care in the outpatient context for the purpose of an interdisciplinary management by networking with various professional disciplines. In the treatment of Long-Covid the call for further supportive and helpful forms of therapy is getting louder, especially since the previous therapy options are purely symptomatic and there is still a lack of evidence-based methods (not only diagnostically, but also on the therapeutic and purely orthodox medical level).
Experience over many decades has shown us that orthodox medicine is complementary with naturopathic procedures, even effectively combined. This multidimensional therapy regime sees the person in his entirety and enables a broader therapeutic approach. Thus integrative medicine has been established which combines orthodox medicine with complementary medicine therapies for the benefit of patients.
Many practicing colleagues from different professional disciplines are already increasingly integrating naturopathic therapy methods into their practice. Especially with Long-Covid the need is enormously big, particularly since conventional medical procedures are currently still limited and many medical colleagues – but also patients – would like a further approach.
According to a press release from the city of Munich on 11.03.2022 the Bavarian Funding Initiative now supports a research project for the treatment of Post-Covid with integrative therapy approaches in the Medical Center of Bamberg under the direction of Prof. Dr. med. Jost Langhorst.
Long-Covid Treatment at KfN Munich
At the Hospital for Naturopathic Medicine (KfN) in Munich, one of the largest complementary medical centers in Germany with connection to the Long-Covid network of the city of Munich, the positive effect of hyperthermia therapy on Long-Covid has already been reported in a smaller study under the direction of their chief physician Robert Schmidt(10) (11). It has been shown that some naturopathic therapy options have proven themselves within the framework of an integrative treatment approach. This article now reports on the accumulated experiences of naturopathic therapy procedures for Long-Covid from the Hospital for Naturopathic Medicine.
A detailed anamnesis is crucial whereby the patient should be recorded in his entirety as a human being. This implies his disposition, habits, social environment (private and professional) as well as his mental state(9).
The integrative therapy regime includes orthodox medical evidence-based treatment in combination with structured naturopathic therapy approaches individually adapted to the patient (with his respective complex complaints). From these approaches synergy effects can form, partly also increase. The measures are aimed at a sustained and lasing improvement of the complaints of Long-Covid, thereby improving the quality of life including the possibility of resuming their profession and if necessary also within the framework of a reintegration during the course of time.
Based on the 5 pillars of naturopathy by Sebastian Kneipp (hydrothermo-therapy, therapeutic exercise [physiotherapy], regulatory therapy, nutritional therapy and phytotherapy) in addition to extended naturopathic methods (hyperthermia, drainage procedures such as cupping therapy), regulatory disorders can be treated and the self-healing powers activated. Therefore you can succeed in alleviating the varied and stressful symptoms of LC. The complaints that are in the foreground with LC and often require an inpatient treatment are manifested particularly through massive exhaustion and tiredness, also known as fatigue. Vegetative retuning measures are a main pillar of naturopathic therapeutic measures.
For this purpose moderate whole body hyperthermia has already proven to be helpful after exclusion of contraindications (see Figure 2). Water-filtered infrared radiation (A) continuously supplies heat and generates an artificial fever. The core body temperature is slowly increased to 38.5°C (mild) or up to 40.5°C (moderate)(10). In the heat accumulation phase the increased body temperature is initially maintained for a certain period of time. Subsequently the patients should rest in a quiet environment for several hours, sweat and drink enough fluids (rest phase). The implementation of this form of therapy is also possible in an outpatient setting, but in that case is not (yet) covered by health insurance. Alternatively, fever therapy in an inpatient setting is also possible in the water with a long-known overheating bath according to Schlenz. Among other things through the whole body hyperthermia a retuning and at the same time an immunomodulating effect takes place(10) (11). The vitality is significantly improved in many patients after only 2 treatments(11).
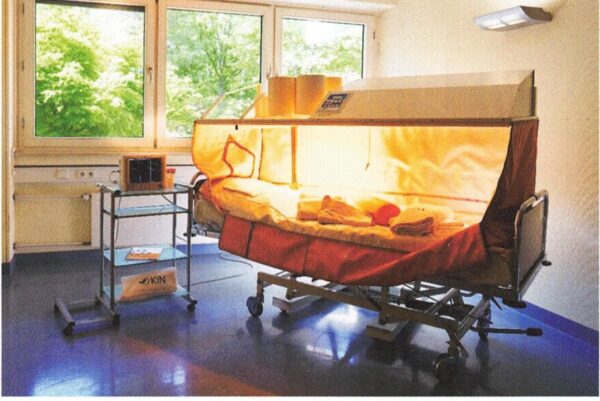 Figure 2: Hyperthermia cubicle at Hospital for Naturopathic Medicine, Munich
Figure 2: Hyperthermia cubicle at Hospital for Naturopathic Medicine, Munich
In the Hospital for Naturopathic Medicine very good experiences with moderate whole-body hyperthermia were already made for many years with various illnesses, especially pronounced states of exhaustion(11). Especially with Long-Covid moderate whole-body hyperthermia integrated into naturopathic complex treatment, still seems to take on a central role(11).
Within the framework of a smaller observational study with a total of 15 patients under the direction of chief physician Robert Schmidt with 12 patients who had received at least one mGKHT after exclusion from contraindications, the first treatment results could already be recorded 4 weeks after full inpatient treatment with the help of self-provided questionnaires. Schmidt and Stange were able to indicate in the case series that the following improvements could be achieved in the 12 patients mentioned with fever therapy regarding a self-assessment of the 3 most frequent symptoms of LC: In 16.7% of the treated patients the state of health improved, and with 9.8% of patients the general quality of life. 15.2% of patients indicated an improvement of muscle pain. In addition to fatigue an improvement tendency appeared furthermore in a whole range of other typical symptoms of Long-Covid(11).
After these positive results of the pilot phase as a basis for further treatment of patients with LC by means of fever therapy and the evaluation with regard to the development of the state of health, an even more elaborate observational study on hyperthermia for LC (over a total of 6 months after the naturopathic complex treatment) is already ongoing at KfN. The goal is to identify other criteria and factors which contribute to a positive effect. Thus according to Schmidt and Stange with a targeted case number of around 300 patients within 2 years if necessary “reliable conclusions” could be drawn about the importance of moderate whole-body hyperthermia for the success of the therapy. The authors explain that this study could, among other things, also provide information about whether mGKHT produces a “significant additional contribution” to the positive effect within the scope of the naturopathic complex program and what influence the number of hyperthermia treatments consequently has on the improvement of the complaints, since only 2 hyperthermia treatments during the inpatient stay have been possible so far due to the pandemic. Furthermore, a higher number of patients within the study could produce further conclusions about the effects of hyperthermia(11). We are eagerly awaiting the results from the larger case series.
Physiotherapy
From the physiotherapeutic side foot reflexology has proven itself. This is a reflective and at the same time regulatory treatment which has a counterbalance and beneficial effect especially in very exhausted patients. Additionally the connective tissue massage comes into question. Reflective techniques also have an immunomodulating effect.
Hydrothermo-therapeutically, cold Kneipp showers [affusions] have proven themselves here, and as a somewhat gentler stimulus the alternating showers for the purpose of retuning, regulatory measures. Sleep inducing, the cold showers are also suitable at night.
Exercise therapy should always be adapted to the individual performance level and not overstretch the curve of the resilience.
With respiratory problems and dyspnea in the context of Long-Covid restrictive changes and susceptibility to infections are often in the foreground. Active participation of patients in the application of naturopathic procedures is required(9).
Physio-therapeutically, respiratory therapy is the focus of the treatments here and it also has a superordinate regulatory therapeutic effect. Respiratory therapy aims to improve the thoracic mobility as well as the respiratory muscles. The physiological breathing rhythm and the direction of breathing are again practiced, so the gas exchange can be improved and thus the secretions can be better dissolved and coughed up(9). At the same time respiratory therapy has a regulatory therapeutic character and has a relaxing and calming effect. With the application of hot cloths, known as “hot rolls” respiratory therapy can be intensified by increasing blood circulation in the area to be treated. Reflective respiratory therapy can be understood as a profound form of respiratory therapy in the sense of a whole body treatment in which breathing is reflectively stimulated by special therapy grips and “tapping massages”. Contraindications to this are osteoporosis, skin diseases, bone metastases and poor general condition.
Connective tissue massage can also be used for reflective spasmolysis (Figure 3). Local hyperemia which is triggered by a shift of the skin can dissolve facial adhesions. Connective tissue massage must not be used in acute inflammation, infections, local thromboses, severe circulatory instability with e.g. syncope, skin diseases, soft tissue metastases, while taking anticoagulants and also not during pregnancy.
Figure 3 showed connective tissue massage with the heading:
Connective tissue massage for reflective spasmolysis.
Treatment methods from the field of osteopathy play a central role in loosening the diaphragm and dissolving adhesions, e.g. craniosacral/visceral therapy.
Even with respiratory problems exercise therapy is recommended with a moderate endurance training 2 x weekly in the sense of Ergometer training adjusted to the performance level, e.g. 25-50 watts for 30 minutes or brisk walking respectively. Breathing trainers (e.g. RC CORNET) in different variants are currently also used to support this.
Muscle tension can be improved by manual therapy, whereby an osteoporosis should be excluded. Supportive craniosacral and fascial treatment approaches with osteopathic techniques are very helpful here. An electrical muscle stimulation treatment with a TENS device can resolve tension and relieve pain. Here the CO2 baths should be mentioned which are used to regulate neuropathic complaints.
Phytotherapy
Phyto-therapeutically and aroma-therapeutically good experiences have been collected with vitalizing rosemary baths in the morning, lavender foot baths to support sleep. Here 5 ml of emulsion are diluted with approximately 4-5 liters of water in a small foot tub.
According to Vogler and Brinkhaus drainage procedures such as cupping massage (bloodless, 2-3 x per week; in the “cupping zones of the chest”) are also described for the treatment of respiratory illnesses(9).
Lemon chest compresses [wraps] have proven themselves phytotherapeutically. Barbara K. Prinz, nursing director of the Hospital for Naturopathic Medicine gives the following instructions: For this purpose a half of an unsprayed lemon is used, and furthermore also beyond that a smaller bowl, a fork, a knife, a glass, an inner cloth, an intermediate cloth (cotton) and an outer cloth (cotton molleton or terry towel). The patient lies on the latter two mentioned cloths which are then used to wrap the thorax. The half lemon is first placed into the bowl, then add approximately 250 ml of hot water so that the ethereal oils do not escape. The lemon is then cut into a star shape [using the fork and knife to release the oils] and squeezed out with the help of the glass. The inner cloth is soaked with the lemon solution, wrung out well and if necessary placed between 2 hot water bottles to keep it warm. The temperature can be checked on the back of the sitting patient before placing the inner cloth onto the chest. It is then applied quickly and as wrinkle-free as possible in the mid-exhalation phase, then the chest is wrapped with the middle cloth and finally with the outer cloth. The wrap remains on the patient’s chest approximately 30-45 minutes, or as long as they tolerate the wrap(14).
From the field of phytotherapy for pain, Phytodolor-Tincture can be prescribed in the dosage
3 x 20-30 drops daily depending on tolerability. The tincture consists of an extract of ash bark, aspen bark and leaves, and goldenrod. The drops are taken diluted in a glass of water with or after eating.
Micronutrients
The need for vitamins and minerals and/or trace elements may perhaps be higher than the daily requirement for a healthy organism(9). For immunomodulation serial high-dose vitamin C infusions are used for several weeks, e.g. 7.5 g diluted in 250 ml NaCl 3 x per week with 1 day break between infusion days or orally with 1 g 3 x daily depending on individual tolerability.
Zinc 10 mg can be prescribed daily for 6 weeks with a subsequent break, as zinc should not be given permanently. In the literature, a dosage of zinc 50 mg daily is also described(13).
In this connection, Schomburg has shown a pronounced selenium deficiency in patients with COVID-19 infection in a study. He describes the “association between severe selenium deficiency and low survival rate” and recommends an adequate supply of selenium for the prevention of diseases(12). Selenium can be given in Long-Covid patients, e.g. at 300 µg per day for 6 weeks, after 2 weeks break can be continued with the same dosage or in reduced form.
Naturopathy
After a COVID-19 infection a large number of patients have smell and taste disorders. Those affected complain about reduced quality of life due to the impairment in everyday life as well as in the social environment. In particularly pronounced forms depressive moods can be the result(13). In their work Hauswald was able to document within 7 months that acupuncture in addition to orthodox medicine has an enormous benefit in the treatment of smell and taste disorders after COVID-19. Thus in the context of the successful study from Hauswald, 70% of the patients were treated successfully.
The immunomodulating effect of probiotics on the nasal mucosa has been known for a long time. In this context the positive effects of treatment with Pro Symbioflor (a bacterial lysate of Enterococcus faecalis and Escherichia coli) in the Hospital for Naturopathic Medicine should be mentioned. The recommended daily dose is 1 drop 2 times daily per side of the nose for several weeks. So far this measure has only recorded isolated improvements, because during the inpatient stay of approximately 10 days some positive course were no longer recorded. A patient with long-standing anosmia was also successfully treated with Pro Symbioflor within the framework of the naturopathic complex program. Perhaps further investigations and studies could bring interesting results, since according to recent studies the number of patients with persistent smell and taste disorders after COVID-19 is increasing(6) (7).
Coping with the illness can be supported with regulatory therapy. Here patients are instructed to actively employ a healthier lifestyle and to avoid overloading (pacing). In the course of an increase in self-effectiveness regulatory therapy has a considerable part in the activation of their very own resources. It thus contributes to the improvement of the overall symptomatology, e.g. by both learning mindfulness and accepting the current status through a positive attitude(9) (15).
Homeopathy
Homeopathy is another indispensable pillar of integrative medicine. Especially organotropic remedies have a good effect in combination with naturopathic procedures, some of which are mentioned here:
For pronounced weakness Acidum phosphoricum D12 can be absolutely helpful. A dry irritant cough can be treated with Rumex D12, a dry, spasmodic cough rather at night with Drosera D12. If ropy, viscous excretions are added Kalium bichromicum D12 is given. With limb pain Eupatorium perfoliatum D12 has proven itself, Cocculus D12 for dizziness. Nocturnal leg cramps can be treated well with Cuprum metallicum D12. Spigelia D12 has been shown to be helpful for headaches, especially with pain above the left eye and radiating into the eye sockets. Furthermore, Gelsemium D12 is suitable for helmet-like pain starting from the back of the head. For sleep disorders with circles of thoughts, Coffea D12 helps at night.
The remedies can be given in the form of 5 globules in potency D12 up to 3 times a day for 2-3 weeks, as long as the symptoms persist.
Outlook
Further studies are urgently needed to establish evidence-based diagnosis and treatment of Long-Covid, equally in the field of orthodox and complementary medicine. Only in this way can a thorough and successful treatment of the many patients with Long-Covid also succeed in the long term.
Conflict of Interest
The author states that there is no conflict of interest.

An Exclusive Translated Article for P2P Supporters
From the Monthly Publications of P2P
Published January 2023
From an article in Erfahrungsheilkunde, Volume 71, Issue #5, 2022
Machine Translation by Lernout & Hauspie, LogoMedia & Promt
Translation & redaction by: Carolyn L. Winsor, P2P Consulting
© Copyright 2022, EHK 2022; 71:275-282 C 2022. Thieme. All rights reserved.
EHK 71; 2022: 275-282
DOI 10.1055/a-1840-8792
ISSN 0014-0082
C 2022. Thieme. All rights reserved.
Karl F. Haug Verlag in MVS Medizinverlage Stuttgart GmbH & Co.
KG, Oswald-Hesse-Straße 50,70469 Stuttgart Germany

Literature
- Koczulla AR, Ankermann T, Behrends U et S1 Leitlinie Post-COVID/Long-COVID. Pneumologie 2021; 75(11): 869-900
- Pink I, Welte T. Häufigkeit, Spektrum und Risikofaktoren von Long-COVID. Inn Med 2022; 63: 813-818
- Petersen EL, Goßling A. Adam G et al. Multi-organ assessment in mainly non-hospitalized individuals after SARS-C0V-2 infection. The Hamburg City Health Study COVID programme. Eur Heart J 2022; 43(11): 1124-1137
- Sommer N, Schmeck Pulmonale Manifestationen bei Long-COVID. Inn Med 2022; 63(8): 819-829
- Hennings JK, Huwe M, Hennings A et al. Respiratory muscle dysfunktion in long-COVID patients. Infektion Doi:10.1007/s15010-022-01840-9
- Ott C. Langfristiger Verlust von Geruch oder Geschmack nach SARS-CoV-2: Millionen betroffen. Ärzte Z 2022
- Tan B. Prognosis and persistence of smell and taste dysfunction in patients with COVID-19: Meta-analysis with parametric cure modelling of recovery curves. BMJ 2022; 378: e069503
- Bauernfeind S, Schmidt B. Stellenwert der COVID-19-Impfung im Kontext von Long-COVID. Inn Med 2022; 63: 840-850
- Vogler B, Brinkhaus B. Kursbuch Naturheilverfahren. 2.Aufl. Göttingen: Elsevier; 2017
- Stange R. Hyperthermie – eine Behandlungsmöglichkeit bei Long-Covid? Z Komplmed 2022; 14(02):44-50
- Schmidt R, Stange R. Erste Erfahrungen mit dem Long-Covid-Syndrom im Krankenhaus für Naturheilweisen in München. Z Komplmed 2022; 14(02): 52-55
- Schomburg L. Update zur Bedeutung von Selen und Selenproteinen bei Covid-19. Z Komplmed 2022; 14(02): 38-42
- Hauswald B. Riechen und Schmecken nach Z Komplmed 2022; [im Druck]
- Prinz BK. Naturheilkundliche Anwendungen in der Pflege. Heidelberg: Springer; 2020
- Rampp T, Kerckhoff A. Was tun bei Post-COVID. Selbsthilfe bei postviralen Beschwerden. Essen: Carstens-Stiftung; 2021
")
