
How to Treat with Long Lasting Success
Or: How do I get the Black Belt in BioResonance?
Dear Colleagues, Ladies and Gentlemen,
Those in our profession are always trained and certified at the most up-to-date level of knowledge through regular advanced continuing education and are challenged anew to prove these qualifications over and over again in the everyday practice with patients. Now however the topic of “BioResonance” provides a great challenge to the user hungry for knowledge. All existing explanatory scientific models are just exactly that, what they are: Models! This means: We form an image of that which could be, admittedly a biologically plausible image, but just “only” an image with the character of a model. We do not know 100% exactly how BioResonance application functions, however we do know that it functions.
And thus we are already right in the middle of the discussion about the scientific materialistic-reductionist paradigm (→ everything can be explained and described from right into the smallest inside / the dominant university approach in today’s school [orthodox] medicine) versus scientific empiricism (→ experiential medicine in the best sense is reproducible and learnable, often however in the absence of research the quintessence is not yet explainable in the sense of the materialistic-reductionist way of thought).
Michael Galle, DSc, HP, biologist and for me a very respected colleague, has described this and much more very well in his publications, and I strongly recommend these to every therapist who would like to use BioResonance.
 Let us note: Year after year in the Fall if I see apples falling out of the tree onto the ground, then I do not necessarily have to be able to explain the materialistic-reductionist earth’s gravitation in order to be able to accept (therapeutically) that also during the coming years in the Fall the apples will not climb into the Heavens, but rather according to experience (empirical-experiential medicine) will fall onto the ground. But of course everybody longs for the day in which we finally find out for certain which electromagnetic oscillations in BioResonance Therapy can influence and control exactly which extra- and intracellular processes.
Let us note: Year after year in the Fall if I see apples falling out of the tree onto the ground, then I do not necessarily have to be able to explain the materialistic-reductionist earth’s gravitation in order to be able to accept (therapeutically) that also during the coming years in the Fall the apples will not climb into the Heavens, but rather according to experience (empirical-experiential medicine) will fall onto the ground. But of course everybody longs for the day in which we finally find out for certain which electromagnetic oscillations in BioResonance Therapy can influence and control exactly which extra- and intracellular processes.
Against this background and apart from the research of Fritz-Albert Popp and Bruce Lipton already another landmark was laid for us “Frequency Therapists”: In 2012 a Nobel Prize for Chemistry was given to Robert Lefkowitz and Brian Kobilka from the USA. They investigated receptors in the body’s cells which process external stimuli, possibly in the form of chemical compounds or light.
Thus here an exactly definable anatomical structure is claimed so that a specific function must exist. Marvelous!
Thus we continue waiting until whenever the next discoveries about the explainability of BioResonance reach us, and for now we turn to the scientific-medical empiricism of BioResonance.
The Most Important Therapeutic Element
Now what is the most important therapeutic element in BioResonance application? The so called “Knock Out Criterion” which in the meantime decides whether or – alternatively – not the treatment runs successfully? The reply to this question is simple and results from the name “BioResonance”: “Bios” is life and “Resonance” in our case here means electromagnetic communication.
So the effectiveness of BioResonance is decisively dependent on how precisely you succeed in exchanging therapeutically effective information (= electromagnetic oscillations) with the body of the patient through a “communicator” (= BioResonance device), which is then forwarded to the receptors of the cell membrane on the inside of the cell, where . . . well, we simply say . . . where they do good there.
We also know examples of specific BioResonance application from Mother Nature: Even if we only think of the frequency spectrum of sunlight and the resonance-conditioned tanning of the skin or Vitamin D formation.
Following these two models we should also be successful in offering effective(!) oscillations to the patients.
In my BioResonance seminars, I always lead with the words: “I am a Heilpraktiker not a Heiltheoretiker* . . . however a bit of theory never hurts.”
Therefore I must describe a little specific theory here, but I promise you high and holy it does not serve an end in itself or the need to complicate anything, but rather it should lead exclusively to the fact that the most lasting therapeutic result is secured with every application.
I would like to begin with the testimony that I deal with BioResonance exclusively in the classical sense. Simplistically said this means that our patients are directly connected by body electrodes and cables with a physically existent BioResonance device. Absolutely there are also other forms of frequency therapy which use the term “BioResonance”, but I simply do not talk about them in the following [article].
We designate the preceding example with the reactions of the body to sunlight as exogenous BioResonance. The patient is simply supplied with frequencies which originated outside the patient’s body and which cause a reaction. In the classical exogenous BioResonance application, a solid or liquid body material of the patient is supplied into the so called “Input Beaker” **. The name “Input Beaker” by the way derives from the fact that the electromagnetic oscillations of the inserted materials are measured and led into the BioResonance device. The more the inserted biomaterial corresponds to the pathology of the patient, the better the therapy result is.
In classical BioResonance Therapy the patient is in direct skin contact with the electrodes, and we designate this as endogenous BioResonance. Here direct electromagnetic potentials from the skin’s surface are measured, are led into the BioResonance device and from there are transmitted as therapy oscillations back through the cables and contact electrodes to the skin of the patients,
In a physical sense an oscillation exists as frequency and amplitude. Now you can easily imagine that we measure no single frequency from the skin of the patients, but rather very many so called frequency sums are transmitted. Here I agree with Alexander Popp (Quote: “As of today it cannot yet be specifically determined which chemical reaction is released in the cell by which frequency. Hence for me it only makes sense to treat with an as wide as possible spectrum.”) As long as we do not know just yet, exactly which metabolism processes in the human body can be controlled with which single frequency; we work with frequency sums which are empirically known to achieve the intended therapeutic effect.
As already suggested classical endogenous BioResonance therapy is operated through body electrodes. Standard are hand and/or foot electrodes, tape and rubber electrodes [non-adhesive flexible electrodes] as well as the adhesive electrodes from ECG diagnostics. The application of the electrodes to the body results according to anatomical conformity, but also according to other considerations, thus e.g. to meridian courses, Head’s zones, painful points, etc.
Therefore after the patient is connected to the BioResonance device with the body electrodes, and also the corresponding body materials (e.g. urine, saliva, blood, operation material, tears, skin chafing, etc.) are inserted into the Input Beaker, the BioResonance device should work. But how?
The devices have various electronic filters built-in in order to extract and to form the best possible electronically filtered and therapeutically effective electromagnetic oscillations from the patient’s presented oscillations. These are then led to the patient’s contact through the Output of the devices.
In the prevailing stages of further development of BioResonance devices, nearly all the manufacturers offer a more or less greater number of so called indications or fixed programs. To the greatest possible extent, these programs consist of preset frequency filters, frequency formation defaults, amplitude settings, etc. for the therapy oscillations. In most cases these programs are collected through positive experiences of many therapists with just those therapy settings on the device for specific indications.
Erich Rasche, with whom I was allowed at that time to learn my basics in BioResonance Therapy, always described this fixed program therapy as the so called “Buckshot Therapy” – therefore a few balls always hit; nevertheless the question is whether the [target] disc falls.
Obviously, the advantage of fixed program therapy is that the therapy in the device runs automatically, as soon as the indications are input and the programs started. Thus this form of application is also easily delegable from the physician or naturopath to “helping hands”.
However what must one do to get from “Buckshot Therapy” to “specific” BioResonance therapy?
BioResonance Therapist = Sound Director
For an easier understanding, I would like to call on your imagination and introduce you to an explanatory picture, exactly how I also try to explain it to my patients in my practice: A singer stands on the stage and sings into her cable microphone. The microphone leads the sung information further to the mixing desk of the sound director. With the result that only just at this mixing desk the sound director has fulfilled all the possibilities to electronically improve the electromagnetic oscillations of the voice of the singer. Then the electromagnetic oscillations released by the sound director are put to the output of the mixing desk and reach from there across the circuits to the loudspeakers (= the body electrodes) and the patient’s bodies can “listen” to the therapy frequencies, just like the concertgoer to the singer.
Of course the singer should be good, but if the voice is “ill” or no good acoustics prevail in the concert hall, then it just needs a perfectly trained sound engineer who ensures the bad (= pathological) transmission of the voice into the room.
Dear Reader, you notice that we are heading for the “K.O. Criteria” of an effective and lasting BioResonance Therapy: The optimal resonance between the singer and the concert public in the great concert hall of the human body, as well as the virtuoso use of the mixing desk by the sound director. The deficient “acoustics” in the body are well explained thanks to the teaching of Pischinger about the functional unity of the interstitial space and are proved anew in everyday practice over and over again: The stronger the over-acidification and oxidation of the interstitial spaces seems, the worse are the “acoustics”.
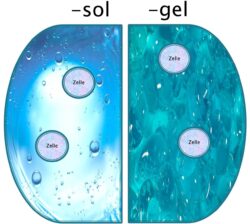 Sol- and Gel- status according to Pischinger
Sol- and Gel- status according to Pischinger
Imagine yourself in a concert hall which is filled with balls on which H+ appears, thus hydrogen – there the sound director must already turn up the volume really well, so that the song comes over the loudspeakers to the people. In this connection the sound quality will nevertheless be absolutely worse than in a “clear” concert hall transmitted to the body: in an environment in which the ground regulation according to Pischinger functions perfectly.
Therefore the central question about the topic of effective BioResonance Therapy
can only be:
Which settings on the “mixing desk” (= BioResonance device) must be selected so that at every moment of the “concert” (= therapy session) the “listener” (= cell receptors for the electromagnetic oscillations) of the “Song” (= therapy oscillations) can reasonably hear, understand and transform?
In order to find these settings the sound director uses his hearing and his experience. However the BioResonance user needs a test procedure (Electro-Acupuncture According to Voll [EAV] or related procedure or as the case may be Kinesiology or Biotensor) in order to measure out the relevant parameters in the patient and to individualize the therapy program. From the “Buckshot Therapy” comes a specific BioResonance application.
The Black Belt of BioResonance
No Question: He who masters these techniques, or at least one of them and can reliably apply them to the patient and to the device, has the Black Belt in BioResonance Therapy and with a reliability bordering on probability also a whole lot of contented patients and accompanied with that an economically well off practice structure.
On the other hand in a figurative sense this means, through various advanced trainings which are device specific offered mostly by the device manufacturers in the BioResonance scene, that you can bring the sound director to the mixing desk in order to be able to individually set the BioResonance device optimally for each patient.
No pain no gain, may we now imagine the one or the other – and this is also correct of course!
Now if suitable seminars are attended, the necessary practice is made and a reassuring routine in measurement procedures has appeared, then he can start off on patients in the practice.
The patient is examined, measured, the parameters of the therapy programs are set and then these are started. Such programs usually run a few minutes, but can however also (one calls them “chain” programs) last from 20 to 30 minutes. According to the version of the respective “BioResonance School” (device manufacturer), at which one feels in good hands. Within these run times of the individualized therapy programs the set values remain constant. You could also say: That the program just remains “monotonous” after its individualization, nothing more changes until the end of the program is reached.
Basically, every classical BioResonance Therapy is an individual therapy, because it works with the body’s own frequencies. When Paul Small is connected he is treated with his own electromagnetic oscillations and not with those from Lisa Miller from the therapy session before [Provided – of course! – that the contact electrodes are changed or cleaned every time between patients! CLW].
But then who says that the parameters set at the beginning after a certain therapy time are still what the body needs to go into resonance and with that into regulation?
For this please imagine yourself once in a seminar, which you want to, or have to, listen to over a long period of time. The lecturer always speaks to you on and on evenly without any change in his vocal situation or vocal color . . . sometimes even the most inclined listener is no longer completely with the subject.
This means: The longer a fixed program with preset, or nevertheless also individualized parameters runs, the greater becomes the probability that the relationship of the offered parameters and actually required parameters breaks apart more and more like scissors.
Then the solution must be:
- Therapy program sequences must be relatively short, and
- Each new sequence must be measured anew in the patient with regard to the necessary parameters, and
- The respective new measurements represent the program parameters for calibration, and at the same time also represent a result value with which the effect on the patient of the preceding BioResonance application can be described and explained
This is quite surely and certainly the Black Belt in classical BioResonance Therapy. I have also worked with the patients in such a manner myself over the years on my own BioResonance device and have brought colleagues into the subject. Then with this practice in my seminars I have almost always seen eager physicians and naturopaths, and today many of them work with this individualizing concept.
Unfortunately however, very many of those certainly interested in device purchase have not reached the Black Belt from lack of time and sometimes perhaps also from lack of patience, and have gotten into BioResonance close combat with patients with a different colored belt. Then in such a manner of course you also gain a lot of time, but the huge number of used devices on the market speaks an eloquent language, and makes one suspect that the attractiveness of BioResonance would like to be measured only in victories.
Unfortunately the individualization concept has a catch!
You must not only learn BioResonance, but also the test procedures (if you have not already mastered this). In order to always offer the body the “correct” BioResonance parameters relevant to the present time, I have checked and customized the actual values over and over again with manual measurements. With one or two patients per day this action may be acceptable. However with more sessions it can rather quickly become strenuous and tiring.
Quintessence
Thus if it is possible through manual measurements on the patient to individually control the respective BioResonance device in the best way possible (similar to a [manual] gearshift with which you can get the best possible performance out of a car), then there must also be the possibility to control this individualization through automatic measurements of the patients (synonymous with a high performance automatic transmission).
Now whether it is Biotensor, Kinesiology or Electro-Acupuncture, every single measurement method is similar to a language and respectively has its own semantics and its own syntax. If [the device] is capable of recognizing this conformity and of transmitting onto others procedures – automatically – in the end you would have a system which through repeated measurements of the patients automatically selects the corresponding parameters and [then] treats. Such a self-calibrating BioResonance device frees you from the pressure of manual implementation, and thus you can make the logic of the Black Belt in BioResonance available for nearly every physician and naturopath – then it doesn’t matter whether or not he has additional qualifications in vegetative testing procedures. Also, the previously affectionately mentioned “helping hands” in the practice get full access at top of the art of BioResonance Therapy.
Dear reader, even with such a self-calibrating BioResonance device, the daily work with patients remains interesting, and unfortunately – I admit this openly – in spite of our best intentions sometimes also less successfully. This then also allows a naturopath now in his 17th professional year to be modest in the evaluation of his own abilities; but at the same time we refer to our motivations and further development in the values and learning from – yes – also from a more or less large number of therapy failures. There are these in all practices, with all methods, and with all healing experts. But with each day we start everything anew to let these aforesaid numbers shrink toward zero.
In this sense I thank you for your time which you have dedicated to reading this article, and I am available anytime for contact and lectures.
![]()

P.S. It has weighed heavily on my mind before deliberately mentioning within the writing of this article that I am the therapeutic developer of the KINDLING EASY. But because you worked this out anyway, I can also just as well say it at this point . . . I am very glad to have found a famous manufacturer who can transform my therapeutic approach into a device that hopefully also brings the world of BioResonance nearer to those therapists who have not yet “dared to approach”. I wish you all a lot of success with BioResonance Therapy in your practice!
 An Exclusive Translated Article for OIRF Supporters
An Exclusive Translated Article for OIRF Supporters
From THE BRIDGE Newsletter of OIRF
Published December 2015
From an article in Kindling BioEnergetik, Sept. 2015
Machine Translation by SYSTRAN, Lernout & Hauspie, LogoMedia & Promt
Translation & redaction by: Carolyn L. Winsor, OIRF
© Copyright 2014, Dr. Uwe Uellendahl, Neunkirchen-Seelscheid, Germany
Note from OIRF: the Kindling EASY is not an OIRF recommended device. However, if you feel this device will work well in your practice, be sure to mention OIRF when you contact Kindling or their distributors. You may then receive a small discount off the purchase price.
For further information on the Kindling EASY, please mention OIRF when you contact:
Mr. Eduard Abrams
Kindling GmbH Medizintechnik
Website: www.kindling.de/eng/

Footnotes:
* This is a “play on words”: Heilpraktiker in German is our Naturopath. Here, however he is saying that he is a natural healing practitioner rather than a natural healing theoretician! Good one, Uwe!
** Also called the input cup (electrode)
")
