
BioResonance According to
Dr. Cornelissen in the
Diagnostics Of Dementia
According to Dr. Cornelissen (1) most dementia illnesses as well as most heart, circulation and cancer illnesses constitute civilization related illnesses. Therefore the main causes of dementias are chemical and/or physical burdens on the organs through the environment or food, and a stress related overloading of the endogenic, physiological regularization systems. These factors lead to metabolic dysbalances and subsequently to degenerative damages. Genetic risk factors merely favor the illness. Exceptions for example are familial Alzheimer dementia, which clearly starts earlier than the much more frequent, sporadic Alzheimer dementia and with which genetic factors play a big role.

Under dementia, lengthy persistent disturbances of cognitive functions in particular memories with otherwise consciousness-clear persons are to be understood. The most frequent forms of dementia are degenerative dementias, and here Alzheimer dementia is the most important. The second most important form is vascular, circulatory related dementias (2).
What importance metabolic dysbalances, life style and environmental toxins have on the origin or the regulation of the early stages of dementia is shown in an actual case study from the University of California (3).
A comprehensive lifestyle and nutrition changeover with sufficient sleep, movement and supplementation of essential materials proved well suited for therapy. In the study from them it is assumed that the combination of several factors in the functional network of the illness events showed a more positive effect than only individual ones. After 3 to 6 months there came an improvement with 9 out of 10 participants with regard to their memory performance. Only one patient in a very late Alzheimer stage did not react to the measures. Six participants had given up their jobs on account of declining memory, or at least had problems with their job. After the treatment everybody was able to work again or to improve their job.
The therapeutic measures in the study included:
- A diet with anti-inflammatory food, simple carbohydrates and avoiding a late dinner
- Insulin monitoring
- Stress reducing exercises, sports
- Mental training
- Reduction of the homocysteine levels with among other things methylcobalamine
- A dose of Vitamin B12
- Balancing of the levels of the different hormones
- Reduction of the amyloid plaques, e.g. with curcuma
- Supplementation with vitamin D3 and K2
- Supply of structural components for the formation of synapses, like e.g. CDP-choline and dehydroascorbic acid (DHA)
- Optimization of the antioxidants and the zinc-copper relationship
- Guarantee of sufficient respiration/oxygen supply during the nighttime sleep
- The optimization of the function of the mitochondria, among other things with Coenzyme Q10
- Supply of pantothenic acid for acetylcholine synthesis
- Exclusion of heavy metal toxins, and
- A dose of medium-chain triglycerides.
Ketones as an Alternative Energy Source
Medium-chain triglycerides are water soluble and without any help from the bilious acid and the pancreas lipase in the digestive system reach directly through the portal vein system to the liver, where they are increasingly metabolized into ketone bodies (4). Ketone bodies can replace glucose as energy carriers in the brain, because often glucose utilization in the brain is damaged very early with dementia, depending on the brain region and the genesis of the dementia (5). With smooth-running ketone bodies the brain receives an alternative energy source for glucose, which moreover is especially energy rich.
A study with a special ketogenic substance (a composition of glycerin and caprylic acid, the latter component in coconut oil: a medium-chain triglyceride) supports this theory. However the effect was rather weak with this mixture (6). By contrast the results of Mary T. Newport were impressive. She gave her husband who suffered from Alzheimer several tablespoons of coconut oil in his food and after 37 days astonishing progress had already been made. Now for example he could outline the dial of a clock (► Figure 1-3) which was not possible for him before (7, 8). Although here this is only about one single case example, something speaks in favor of it (3, 9) that with nutrition with medium-chain triglycerides various positive effects are to be expected on the course of a dementia.
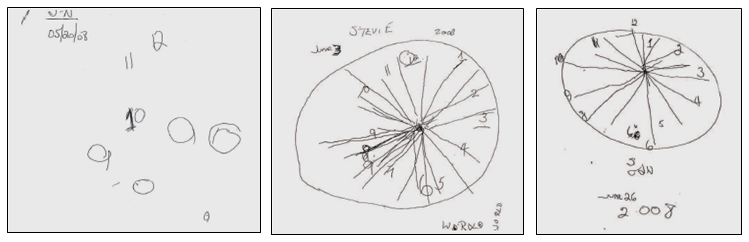 Figure 1-3: The American physician, Mary T. Newport had her husband [who was] ill with dementia draw out the dial of a clock from memory – a widely used test to determine the severity degree of a dementia. The illustration makes clear that for him the Ketone Cure showed an astonishing effect. Left: One day before the beginning of the therapy. Center: After the first two weeks. Right: after 37 days taking the coconut oil. © VAK Verlags GmbH
Figure 1-3: The American physician, Mary T. Newport had her husband [who was] ill with dementia draw out the dial of a clock from memory – a widely used test to determine the severity degree of a dementia. The illustration makes clear that for him the Ketone Cure showed an astonishing effect. Left: One day before the beginning of the therapy. Center: After the first two weeks. Right: after 37 days taking the coconut oil. © VAK Verlags GmbH
Besides medium-chain triglycerides other alternative energy carriers than glucose are also promising candidates to supply the brain. Galactose, for example can be taken by insulin dependent [patients] and in a method independent of insulin in the cells (liver, brain, muscle). As a result, after the metabolization of galactose (in comparison to glucose) nitrogen-containing amino acids occur whose production especially promotes the reduction of ammonia. At the same time with this the highly toxic ammonia is decontaminated from the brain (10). Clinical studies for galactose and dementia in people are apparently still absent.
 Medium-chained triglycerides contained in
Medium-chained triglycerides contained in
coconut oil can be used in certain cases for
alternative energy production in the brain.
Causes of Dementia
Now let us look at the most important specific burdens which according to Dr. Cornelissen can be considered as the cause of dementia, and which lead in particular to a longer continuing effect for indirect or direct damage to the brain (1):
Faulty Nutrition
Faulty nutrition displaces the natural intestinal flora. Increased growth of Candida-yeast-fungi occurs which forms the toxic acetaldehyde. Acetaldehyde, which the body cannot sufficiently eliminate or neutralize, burdens the brain in particular in the Corpus callosum, responsible for the integration of the left and right brain hemispheres as well as the coordination of the emotions and understanding.
A longer sustained Candida burden is accompanied on a continuing basis by decomposed flora (leading group Clostridium), which again generates ammonia in excess as a byproduct, which is likewise toxic in the brain and in particular has an effect here in the Hippocampus. According to Dr. Cornelissen ammonia is a high promoter of aging dementia.
Cortisol
The hormone cortisol from the adrenal gland is a typical stress hormone. It activates catabolic metabolism processes and thereby makes glucose available for the body in sufficient amounts from the reserves of the organism. The main cause of prolonged increased cortisol values is chronic stress. With older people who suffer from dementia cortisol is often found raised. Continuously raised cortisol values above all damage the Hippocampus, which in particular possesses many receptors for this hormone. The Hippocampus plays a special role in the genesis of dementia because it represents the interface between short term memory and long term memory.
Arteriosclerosis
Deposits and constrictions in the brain arteries, as they especially appear with vascular dementia, result among other things in a poor supply of glucose in the brain cells. The energy is missing for all necessary nervous functions, thus also the energy for formation of the important neurotransmitter acetycholine which is then produced in a small quantity.
Gluten Intolerance
With a gluten intolerance the grain protein can be taken in with the nutrition which passes the intestinal wall and reaches into the central nervous system through the blood/brain barrier where it results in allergo-toxic reactions which express themselves in different psychosomatic disturbances. On the other hand milk protein is rather unobtrusive.
Environmental Pollutants
According to the experiential values of Dr. Cornelissen there are no dementias without a clear burden through environmental toxins. Organic connections (e.g. PCP, PCB, DDT, formaldehyde, methanol) belong to the neurotoxically relevant environmental toxins. In addition heavy metals play a role which make the blood/brain barrier coarsely meshed and thus generally more permeable for toxins. Important toxic heavy metals in the order with respect to the relevance of their significance are: cadmium, lead, arsenic and mercury.
Therefore to sum up, it should be emphasized that all dementia relevant substances (acetaldehyde, ammonia, cortisol and acetylcholine) can be recorded with the MORA® System. Also included in the MORA® test system are the important brain areas like the Hippocampus, Lobus frontalis and Lobus temporalis.
Diagnosis with MORA® BioResonance
For diagnosis the relevant burdens are identified non-invasively through the MORA® BioResonance according to Dr. Cornelissen. With the burdens it concerns a two way choice about the noxae, which critical concentrations are surpassed or are too little, as well as too many essential substances, like for example nutrients, minerals, vitamins or hormones. Moreover all brain areas are tested for their degenerative state. As a special feature of the MORA® BioResonance the burden can be associated (filtered) with the relevant brain area. In addition the strength (importance) of the burden is measured, from which the therapy is derived and which begins in each case with the strongest burden. A diagnosis and therapy with regard to dementia should always be preceded by a MORA® System Diagnostic for the recording of the total condition of the organism. Important steps of the MORA® Dementia Diagnosis and Therapy (1) are:
All brain areas are tested as far as their degenerative state. For example, for Alzheimer illness the medial areas of the temporal lobes (Hippocampus and entorhinal cortex, deep inside behind the ear) are injured first. A corresponding symptom is the disturbance of the transition of short term memories into long term memory. Furthermore special attention is given to the temporal lobe and the frontal lobe of the cerebrum. Disturbances in these sectors influence associative as well as causal thinking.
A deficiency of the important neurotransmitter for stimuli transmission, the acetylcholine shows as a burden first in the sectors of the Hippocampus, temporal lobe and frontal lobe. As well it can be tested on the preliminary stage of the acetylcholine, the dimethylaminoethanol (DMAE). The substitution of acetycholine over this preliminary stage presents itself as a therapy.
A marker for a burden of the vessels is raised homocysteine levels which among other things produce malnutrition, if there are certain vitamins (B12, B6 and B9) lacking. The result is vascular damage which limits the supply of nerve cells through the inhibition of the cerebral blood circulation. Homocysteine has an effect directly on the neurotoxic and neurodegenerative and is accompanied by psychic symptoms like restlessness, discontent and depression. Here we either test the deficiency indirectly on the corresponding vitamins or directly with the homocysteine preparation, in that we filter the homocysteine tested as a burden over the also positively tested brain arteries. In addition the problem-relevant B vitamins are quantified on the basis of deficiency and accordingly substituted together with SAM (S-adenosylmethionine). Nevertheless it should be considered that vitamin B resorption suffers with an intestinal dysbiosis.
All neuro-infectious illnesses should be excluded as a cause of the dementia. Viruses and bacteria (e.g. Borrelia) are determined in the [cerebrospinal] fluid through the corresponding resonance with the technology of the correlation test. Viruses can be treated very well with the MORA® BioResonance.
The toxic acetaldehyde from a burdened intestine has an especially serious effect on the Corpus callosum which integrates both hemispheres (Emotio and Ratio – emotion and rationality). Accordingly this burden is filtered on all brain areas with special attention to the Corpus callosum.
Toxic ammonia from a burdened intestine has an unspecific effect on the whole brain, however the Hippocampus is particularly affected. With dementias with a high ammonia burden the glutamine synthesis is not sufficient. In the brain the glutamic acid detoxifies the ammonia while it is converted by it into glutamine (see galactose above). At the same time arginine is tested in deficiency in the patient. Low glutamic acid values and high ammonia values in the brain can be well tackled with the preparations arginine, glutamine and ornithine-aspartate. The cause of the increased ammonia burden from the intestine should also be treated.
Typical microinflammations, as they appear with all important chronic inflammation illnesses, can be identified while the positively tested brain areas are filtered over arachidonic acid. The most important substances against microinflammations in the brain are Omega-3 fatty acids (with a high proportion of DHA), Alpha lipoic acid and Coenzyme Q10. With dementia after inflammation illnesses, the intestine should additionally be searched. The intestine is in connection with the brain through the nerve fibers. Thus inflammation processes in the intestine also have an effect on the brain.
As further possible burdens for dementia only the burdens of the environment are mentioned here. Especially important E-Smog comes up here, which has an effect on the epiphysis and melatonin is degraded. Testing malondialdehyde has turned out as the general indication to the burden through environmental toxins. Thus if the quantification exceeds a value of V=500 a treatment-deserving environmental burden is present, whose therapy consists of a specific detoxification.
Therapy According to Dr. Cornelissen
The MORA® Therapy for dementia according to Dr. Cornelissen always consists of a supplementation of the required materials and/or their preliminary stages known to be in deficiency. Further support with problems of the brain being in connection with the organs is treating causally like for example the intestine. In addition suitable medication against the different forms of dementia can be individually tested. An amplification of over 20, obtained with the efficiency measurement characterizes a good medication, over 40 is excellent. The special advantage of MORA® BioResonance Diagnostic according to Dr. Cornelissen lies in the individual customized to the patient testing of all burdens and with that the inclusion of the important key factors of the illness events. The patient receives a “tailor-made” therapy plan. Nevertheless, the earlier the therapy is begun, the greater are the chances to already recognize and to regulate present dysbalances in the cerebral metabolism before each morphological change in the brain, and thus to avoid substantial morphological failures.
The rare disease of Auguste D.
A little more than 100 years ago, on the 19th of December, 1915, Alois Alzheimer died, the discoverer of Alzheimer’s, a disease named after him. As one of the few doctors of his time, he searched for the core of the disease, which was so far seen as a purely mental problem.
Disoriented, confused, uncontrolled and caught between emotional extremes – in this condition Auguste Deter was taken to the municipal asylum for lunatics and epileptics in Frankfurt by her in the meantime fully overstretched husband on the 25th of November, 1901. He could neither understand nor prevent that his wife Auguste had changed significantly for approx. half a year: She had recently been hiding things in her own house, without any reason, bothering the neighborhood, suffering from absurd jealousy and fear of acquaintances. Furthermore she could hardly get by in everyday life and had more and more serious memory problems
 Auguste Deter, 1850 – 1906
Auguste Deter, 1850 – 1906
Not only the symptoms per se raised questions. These are often well-known unavoidable complaints of old age. What was extraordinary is that Auguste Deter was not yet 70 or 80, but only 51.
Someone that was particularly interested in this fact was the medical assistant Alois Alzheimer. He concerned himself intensively with the patient and kept extensive and detailed records of her condition. One day after her admission the following dialogue, which meanwhile gained notoriety, took place and showed in its simplicity very pointedly the helplessness of the patient.
Sits up in bed with a puzzled facial expression.
What’s your name?
“Auguste.”
Last name?
“Auguste.”
What’s your husband’s name?
“I think Auguste.”
Your husband?
“Yes so my husband” (apparently did not understand the question.)
Are you married?
“Yes Auguste.”
“How long have you been here for?” (Seems to delve into herself)
“3 weeks.”
“What is this?” (pencil)
“Steel spring.”[1]
After this conversation many others followed and it was clear that Deter became more and more disorientated. Alzheimer confronted her with some calculation tasks, asked her to tell the time or read out a text, continuously asked for her personal data and requested her to write them down. While her answers became more confused, time and again she also lost control over her behavior. Periods of anxiety alternated with periods of passivity as well as restlessness. In these periods she walked through the clinic and touched other patients’ faces, even hitting them, and as a result got hit too. At that time the motives of her actions were completely inscrutable – for outsiders as well as for herself. In one of the conversations she concluded: “I lost myself, so to speak” [2]. It could not have been described more appropriate. Also statements like “I’m so wrong – so wrong” [3], give us a vague idea that her own life at this time must have felt like an incomprehensible labyrinth to Deter.
Auguste Deter died on the 8th of April, 1906. The news of her death also reached Alzheimer, who in the meantime worked in Munich, but had always maintained contact with Frankfurt. He claimed his former patient’s brain and dissected it. In the process he discovered the protein deposits, nowadays called plaques, destroyed fibres and the depletion of brain cells.
The diagnosis before section, as shown in the clinical report, stated “Plain disturbance of the soul” [4]. Alzheimer knew that he could not be content with this and therefore presented the findings of his observations and the investigation of the brain to other doctors on the 3rd of November, 1906. Platform for this was the 37th conference of South West German psychiatrists in Tübingen.
To his great disappointment his lecture on A rare disease of the cerebral cortex did not receive any attention. With a focus on the entourage of the psychoanalyst Sigmund Freud, to be precise on his then comrade C.G. Jung, Alzheimer’s lecture did not give rise to any questions.
Alzheimer himself died, at the age of 51, in 1915. The full recognition of his research on the disease of Auguste Deter was granted only many years later.
Yvonne Dauer,
Research Associate
Med-Tronik, GmbH
- Institut für Stadtgeschichte Frankfurt am Main, Nervenklinik 3580, Bl. 3v (Translation by HOLOS language solutions)
- Institut für Stadtgeschichte Frankfurt am Main, Nervenklinik 3580, Bl. 4v (Translation by HOLOS language solutions)
- Institut für Stadtgeschichte Frankfurt am Main, Nervenklinik 3580, Bl. 10v (Translation by HOLOS language solutions)
- Institut für Stadtgeschichte Frankfurt am Main, Nervenklinik 3580, Bl. 1r (Translation by HOLOS language solutions)
See also: http://thebrain.mcgill.ca/flash/capsules/histoire_jaune03.html
 An Exclusive Translated Article for OIRF Supporters
An Exclusive Translated Article for OIRF Supporters
From THE BRIDGE Newsletter of OIRF
Published October 2016
From an article in Naturheilkunde, July 2016
Machine Translation by SYSTRAN, Lernout & Hauspie, LogoMedia & Promt
Translation & redaction by: Carolyn L. Winsor, OIRF
© Copyright 2016, Cornelissen and Tesmer, Med-Tronik, Friesenheim, Germany


Literature:
- Cornelissen G: Demenz, M. Alzheimer und MORA; in Med-Tronik GmbH (ed): Neurodegeneration und MORA: Frühdiagnostik und Therapie von neurologischen und demenziellen Erkrankungen mittels MORA, pp 2–103.
- de Gruyter: Pschyrembel Online. Berlin, de Gruyter. pschyrembel.de.
- Bredesen DE: Reversal of cognitive decline: A novel therapeutic program. AGING 2014; 6:707–717.
- Aoyama T, Nosaka N, Kasai M: Research on the nutritional characteristics of medium-chain fatty acids. J. Med. Invest. 2007; 54:385–388.
- Hoyer S: Glucose metabolism and insulin receptor signal transduction in Alzheimer disease. Eur J Pharmacol 2004; 490:115–125.
- Henderson ST, Vogel JL, Barr LJ, Garvin F, Jones JJ, Costantini LC: Study of the ketogenic agent AC-1202 in mild to moderate Alzheimer’s disease: a randomized, double-blind, placebocontrolled, multicenter trial. Nutr Metab (Lond) 2009; 6:31. http://www.biomedcentral.com/content/pdf/1743-7075-6-31.pdf?wptouch_preview_theme=enabled.
- Newport MT: Alzheimer’s Desease: What if there was a cure?, 2016. http://www.coconutketones.com/ (accessed June 9, 2016).
- Newport MT: Alzheimer’s disease: What if there was a cure? the story of ketones, 2nd ed. Laguna Beach, C.A., London, Basic Health; Deep [distributor], 2013.
- Wallace DC, FanW, Procaccio V: Mitochondrial energetics and therapeutics. Annu Rev Pathol 2010;5: 297–348.
- Roser M, Josic D, Kontou M, Mosetter K, Maurer P, Reutter W: Metabolism of galactose in the brain and liver of rats and its conversion into glutamate and other amino acids. Journal of neural transmission (Vienna, Austria 1996) 2009; 116:131–139.
Translator’s Notes:
- Ground Regulation System:
- A special report with accurate English translation of a series of seven German language articles initially published by Dr. Heine in 2011.Total of 48 pages with information that is mandatory reading for all practitioners of orthodox and complementary medicine. Available from OIRF in electronic (PDF) or print formats for $30.
- Also see the book: The Extracellular Matrix and Ground Regulation, Basis for a Holistic Biological Medicine; By Alfred Pischinger and Hartmut Heine (available in English on Amazon)
- In my ongoing efforts with the translation work I do for OIRF, it is my goal – my standard – to give you the exact words and meaning of the German author. In other words I consider myself as a translator, and not as an interpreter who would insert their own opinion or “interpretation” to what was said in German. In this article Dr. Cornelissen made a very clear distinction between what he considers a “disturbance” as opposed to a “burden” or “stress” factor. In all cases I have translated his use of each word exactly.
There is a very real difference here in that there can be a “disturbance (field)” in the body (even internally generated), whereas a “burden” or “stress” in this context is primarily an external influence that can or does create a disturbance. The usual translation in the literature tends to haphazardly interchange these terms, but for this article (even though it sometimes doesn’t “read” right in English) I have carefully preserved an exact translation so that you can see Dr. Cornelissen’s meaning. Here the word burden is primarily used in the sense of an external factor which is stressing, polluting or (over)burdening the body. CLW
")
