
We have all learned the standard interpretation of EAV measurement values (see previous article, The Bridge, Vol. 4, Issue #4). These interpretations hold true when most of the measurements are in a normal range (50-64) and stable, but what do we do when all measurements return pathological values? It is not uncommon to find that every “nail” point returns a high value with or without an i.d. If we interpret this according to the standard interpretations then we have to assume that the patient is very unwell – every organ is showing signs of inflammation, yet the patient is sitting there smiling at us and saying that they feel fairly well. What is going on? Our measurements tell us that the patient is unwell; the patient is feeling not too bad. This brings us into the topic of measurement patterns. Assuming that we have a good and reproducible measurement technique then the first thing to look at is the pattern of measurements. For this purpose it is very helpful to display the measurements as a graph.
Before going on to look at some of the common patterns I should point out that it is insufficient to take measurements from only the nail points. Dr Morell insisted that we should measure all of the points on the hands and feet in order to get a sound diagnosis. In principle I agree with this but it is time consuming and it does assume that the practitioner has a detailed knowledge of all of these points. In the first visit I often find that it is sufficient to measure the terminal or “nail” points together with the CMP’s of each meridian.
The first thing that I look at is the overall pattern of measurements obtained from the terminal points. There are several common patterns:
- Normal
- All measurements slightly high
- All measurements very high
- One side of the body showing normal ranges of value, but other side showing high values (Assymetry).
1. Normal
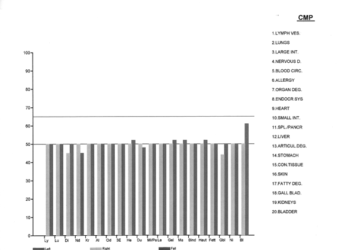
This pattern shows that the majority of measurements lie within a normal range, i.e. between 50 and 64 with stable values. Remember that an i.d. always indicates a problem. There are a few slightly low values which may indicate very minor problems, and one slightly elevated value on the left bladder meridian. There are no indicator drops.
When we see this pattern we should breathe a sigh of relief because the body is telling us where to look. In this example I would take additional measurements from the bladder meridian (highest) and from the gall-bladder meridian (lowest). In the example the patient was feeling very well and had attended for a check-up.
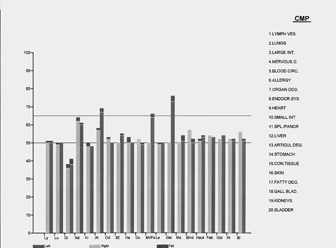
2. Slightly High Measurement Values
By slightly high I mean that the majority of values range between 65-75, with or without an i.d.
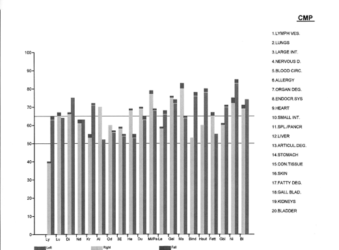
When we see this pattern we should forget about trying to interpret what the medical situation is. We are seeing a picture of a minor overall burden on the body which is disturbing all meridians but which is not necessarily causing major problems. The difficulty is that the pattern is masking the true underlying picture and hence should be treated first.
In this example the patient was complaining of bowel disturbance but the measurement values do not provide a clear picture.
This particular pattern usually indicates a displacement of the TMJ.
The TMJ controls the bite. The lower jaw portion of the joint fits into a fairly shallow notch in the upper jaw portion of the joint. The seating of the joint is easily disturbed leading to misalignment of the jaw. According to Voll, there is a secondary meridian surrounding the jaw which connects to all of the main meridians in the vicinity of the TMJ. Hence, if the TMJ is displaced then it is likely that all meridians will become disturbed. There may not be any obvious symptoms but we will not be able to make a more detailed diagnosis until this problem is corrected.
Correction of the TMJ (at least temporarily) is quite easy. Stand behind the patient and tilt the head backwards so that the patient is looking up. Place both index fingers over the TMJ (left and right). Ask the patient to open and close the mouth. With a little experience one can often feel a difference between the two sides. Next, Place the left hand on the left side of the face pushing slightly against the chin, and the right index finger over the right TMJ. Ask the patient to open the mouth wide and to resist your slight pressure on the chin. Now ask the patient to quickly close the mouth. As they close use a gentle finger pressure over the TMJ. The joint should re-seat itself. The key to success is for the patient to close the mouth very quickly and simultaneously you apply gentle finger pressure over the joint.
Repeat for the other side.
Finally, stand to the side of the patient, tilt the head back and ask them to open wide pushing the chin forward. The practitioner holds the back of the head with one hand and holds chin with the other hand applying a firm pressure towards the crown of the head while the patient quickly closes the mouth.
Very often the practitioner will feel (and hear) a sharp click as the joint slides back into position. It is important not to apply any thrust or violent movement. The practitioner is only applying a resistance; the patient is doing the work. The whole procedure takes only a few seconds and should not cause pain.
After correcting the TMJ then the terminal points should be re-measured. In most cases the values will now have normalised revealing where there is a genuine imbalance.
This graph shows the measurement values from the same patient immediately after adjustment of the TMJ. We clearly see the disturbance in the large intestine meridian left side.
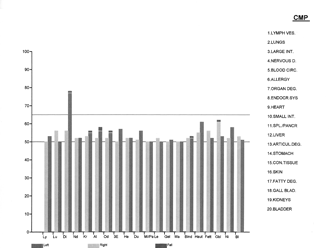
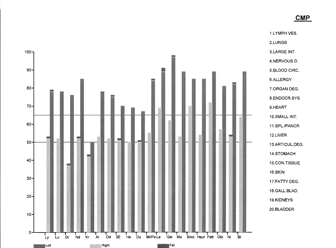
3. All Values High
This pattern is very similar to the previous one except that all values are greater than 70 and very often greater than 80. Again, there may or may not be indicator drops.
This pattern always indicates geopathic or electro-magnetic stress. Both geopathic stress and electromagnetic stress are global stresses. They impose a stress on the whole body even though they may be focussed on one region of the body. The effect of these stresses is that they create false harmonics in the body which can mimic other toxic agents. In addition they almost always create a false polarity. Here, the spin test becomes essential. One should always test both the blood and the urine for spin polarity. In normal circumstances the blood should have a right spin (dextro-rotatory), and the urine should have a left spin (laevo-rotatory). A reversal of blood spin has a high correlation with geopathic stress, and a reversal of urine spin has a high correlation with electro-magnetic stress. If either or both fluids return a reversal of spin then it must be corrected before proceeding with further treatment. The patient should also be advised about the nature of these stresses and preventive measures suggested.
After correcting the spins and treating for geopathic/electromagnetic stress the terminal points should be re-measured. If correct treatment has been given a dramatic improvement in measurement values will be observed. In ideal circumstances most values will now be in the normal range but there will be occasions where after correction of these global factors the values have reduced but not normalised. The pattern that remains is often the TMJ pattern which needs to be corrected.
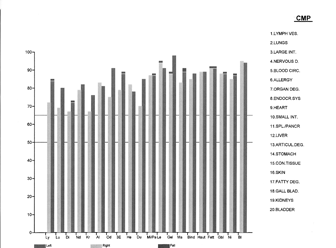
4. Asymmetry
The final pattern that I wish to illustrate is where one side of the body returns normal range measurement values but the opposite side returns pathological values.
These were the resulting measurements from the above patient after treating the geopathic stress. This pattern indicates the existence of a focus on the side of the pathological values. A focus is an area of chronic inflammation that may be asymptomatic in the region of the focus but which is causing distal disturbances and the appearance of symptoms elsewhere in the body. The majority of foci occur in the head – dental, tonsils, and paranasal sinuses. In adults dental foci are by far the most common. These include dental decay, gum problems, and inflammation in the jaw bone. In children, tonsil foci are more common. Sinus foci are also very common in both children and adults.
It should be noted that cranial foci are not the only areas that focal situation can occur. Other very common areas are the appendix, the gall-bladder, and the ovaries although any part of the body can act as a focus.
Treatment of foci is quite difficult and when suspected the patient should be referred to the appropriate specialist unless the practitioner is very experienced. The whole topic of focal disturbances will be the subject of a future article.
Many patients and practitioners are interested in allergies and sensitivities. One very common problem with EAV testing is that we will often find a number of allergies (I use the term allergy in a general sense to include sensitivities). We treat the allergy with desensitising drops with the patient avoiding the allergen for a period of 3-6 weeks. On re-testing we often find that the original allergies now test negative but new ones have come into the picture. This phenomenon of substitution can occur no matter how well we think we are treating the allergies and we never seem to get the patient completely clear. The reason for this is that the immune system is being over-burdened by other causes and the allergies are arising because of that. Until the underlying cause is detected and treated, the patient will not be clear of allergies for any substantial length of time. In most cases the underlying cause is the presence of a focus.
The same patient after the dental focus had been treated. We now see a few remaining problems, the main one being weakness in the large intestine.
It is important to recognise and treat these basic patterns. If we ignore them then we are in danger of making a false diagnosis and of giving incorrect treatment. If we prescribe medications for every point that shows imbalance then we will be over prescribing to the detriment of the patient. The greatest challenge in our work is to be able to devise a suitable treatment plan based on accurate assessment of the case. Recognising and dealing with these patterns of measurement is one of the first steps to be taken.
Please follow this link to see Dr. Scott-Morley’s Part 1 article Taking EAV Measurements.
 An Exclusive Article for Members
An Exclusive Article for Members
From THE BRIDGE Newsletter of OIRF
Published October 2008
© Copyright 2008, Dr. Tony Scott-Morley, UK

")
