
The Phenomena of the Extracellular Matrix
As an Attractor for Waste Products
Summary
The circadian rhythm of the acid-base flooding in the extracellular matrix (ECM) is in feedback as the physiological basis of cell metabolism. The ECM is connected through the sodium chloride cycle to the circadian rhythm of the liver. Deviations from these feedbacks are always connected with a latent acidosis as a starting point for the ‘clogging up with waste products’ of the ECM. This is measurable in a chronic acid pH of the urine. Hence, an exogenic base supply is the focus of therapy.
Key words: Extracellular matrix, acid-base flooding, slag/waste products
Construction and Function of the Extra-Cellular Matrix
The extracellular matrix (ECM; basic substance) is inserted as a molecular sieve into every cell from PG/GAG’s (proteoglycan/glycosaminoglycans), structure glycoproteins (collagen, elastin) and interlinking glycoproteins (among other things fibronectin, laminin). The PG/GAG’s are the structural basic element of the ECM. On the basis of their negative charge, they are capable of binding water and ion exchange. Through the capillaries and the vegetative nerve fibers the ECM is connected to the hormone and central nervous systems. Therefore every somato-psychic and psycho-somatic event is reflected in the organization of the ECM. The ECM is formed peripherally by fibroblasts and centrally by astrocytes. PG/GAG’s structure a porous polysaccharide gel with an enormous surface, through which arises extraordinarily diverse possibilities for the formation of chemical compounds. PG’s also push through the cell membrane and thereby contact the cytoskeleton with effect on the entire cell behavior. They interact non-covalently with the sugar part of the chains, thus a PG pair in this situation is able to hold the weight of approximately 1,600 cells. Together the ECM and the cells form a flexible viscose system that keeps itself in order from the effects of external forces by self-stabilizing (“tensegrity” ◊◊). The ECM thus represents an attractor for all external and internal active forces in the style of linked feathers, by which small causes can have very big effects (2).
Through the connection from silicic acid (Si) to the PG/GAG’s the ECM maintains the function of a “nano-composites membrane”. Therefore the small, like the large, molecules get the same diffusion possibilities. Si has semiconductor properties which are suitable for the interception by radicals under transmission of photons. On the other hand, all cell functions are thus influenced. The PG/GAG’s-Si-complex represents redoxactive macromolecules which are exceptionally sensitive against contaminations, as for example heavy metal ions from the environment. They are coated by a mono-molecularly “tense” water film (“stretched water”) whose energy status can cause many catalyses (2).
Life signifies “stress” in individual time intervals (profession, psyche, environment, nutrition, aging, etc.). Among other things this leads to an increased catecholamine level with reactive qualitative and quantitative change to the ECM components. Among other things it then increases matrix components diminished by activated proteolytic and hydrolytic enzymes. On the other hand synthesized PG’s can intercept increased lipids (e.g. dermatan sulfate protein) (2).The cells react to stress among other things with increased formation of oxygen radicals (ROS). From it originates a pro-inflammatory situation which is accompanied by the increased acute phase proteins and leads to increased production of Tumor Necrosis Factor alpha (TNF-α) from monocytes/macrophages. This leads to glucose utilization disorders (“Insulin resistance”), increased instability of the coagulation system, hyperlipidemia and inclination to chronic inflammations (“metabolic syndrome”). Glucose excess leads to non-enzymatic glycosylation of all sugar components in the ECM (advanced glycation end products, AGE’s). The AGE’s are polymerized by the ROS under inclusion with the lipids into large insoluble molecules. All these “clogged up waste products” in the ECM indicate a process leading into a positive feedback with the danger of developing chronic diseases and tumors (2).
Clogging up and Detoxification as a Physiological Process
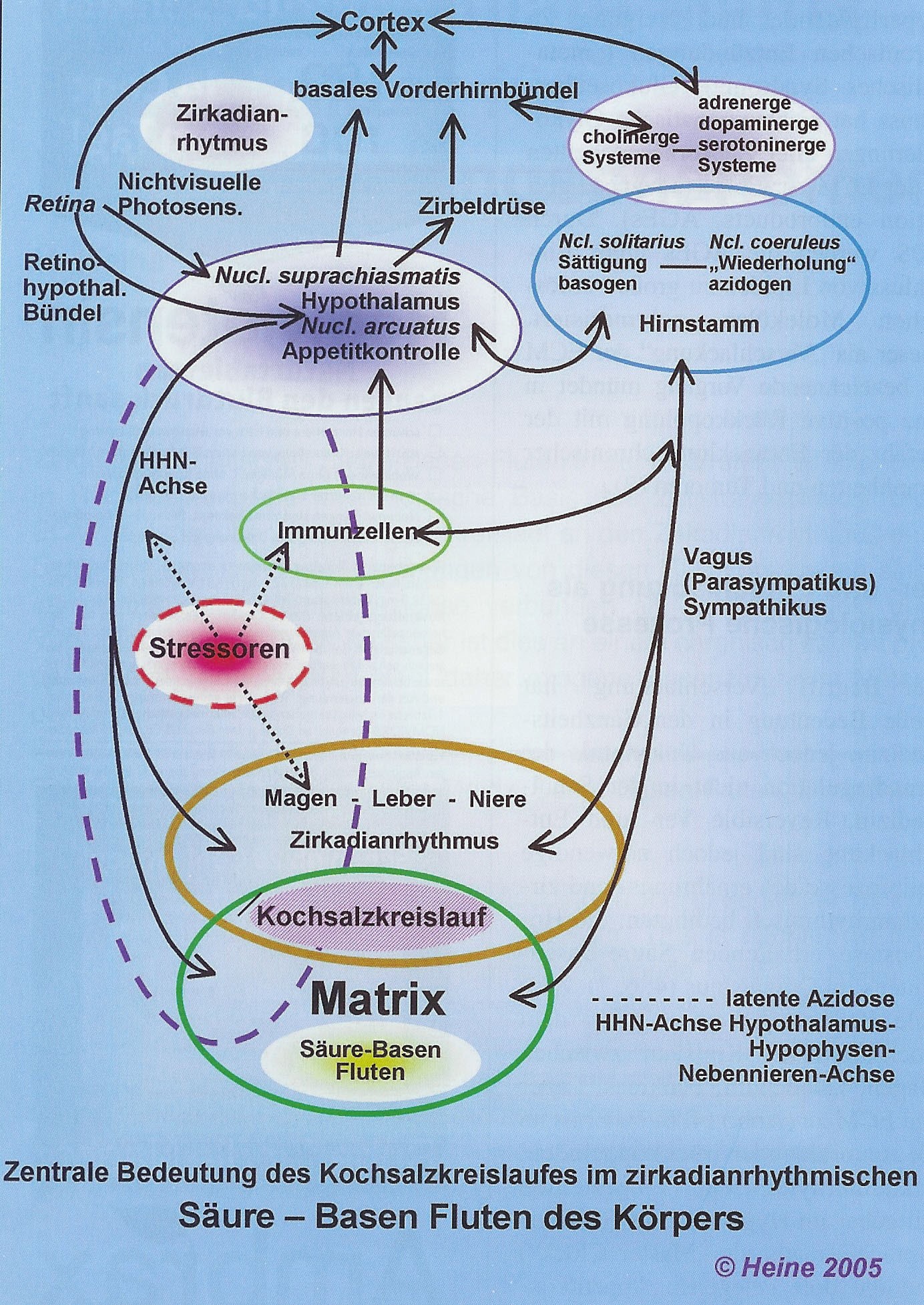
The concept of “clogging up [of the connective tissues with waste products]” has great importance in the entirety of medicine, but not in orthodox medicine because of ignorance of the ground regulation. Reversible clogging up and detoxification cause, however necessary the partial processes of nutrition and circadian rhythm, the maintained homeostasis of the acid-base floods in the organism (4, 6, 7). Besides, central importance comes from the sodium chloride (common salt, NaCl) cycle between stomach, duodenum, pancreas, liver and ECM (Diagram) (4, 6, 7). It is bound to a feedback among themselves, the circadian rhythm adjusted timer in the hypothalamus (suprachiasmatic nucleus as the “Master Clock”) and the appetite control centers located there (arcuate nucleus) (5). These stay in connection with the epiphysis (circadian melatonin formation, sleep-waking rhythm), the saturation center (parasympathetic solitary nucleus) and the sympathetic nucleus caeruleus (“wish for repetition”). From the periphery, afferent vagus fibers of the gastric wall reach the solitary nucleus and stimulate the hunger feeling in the empty stomach (Diagram) (4, 5, 8). In a humoral way, the orexigenic ghrelin peptide (hunger trigger) is formed by the empty stomach from the hydrochloric acid established parietal cells in the stomach mucosa, which works by activating the appetite center in the arcuate nucleus (3).
For a translation of these terms please see the end of this article.
With ingestion, the parietal cells of the stomach glands in the lumen release hydrochloric acid (HCl) leading at the same time in the basolateral gland cell range for release of an equivalent amount of basic sodium hydrogen carbonate (NaHCO3). It reaches into the underlying capillaries and across the blood course into the base dependent bowel and bowel appendix gland (brunner and lieberkühn glands in the duodenum as well as the pancreas and liver). There the NaHCO3 is neutralized by the HCl and arrives back as resynthesized sodium chloride into the blood circulation (8). Whereupon it is once more available to the parietal cells (4).
In principle although food can be taken in arbitrarily, for people it is accepted that he takes his main meal toward the end of the daily center (approximately 1 PM). A deeper meaning comes from it, because synchronically with the starting higher HCl formation in the antiport a maximum "base flood" originates and this coincides with the endogenously caused daily temporal "secretory" phase (about 8 AM to 7 PM) of the circadian liver rhythm. Besides, the enzymatic substances made in the liver (glucose and synthesized bile) which are usually eliminated with the urine are delivered into the blood stream and/or into the duodenum. Vice versa, the "base low flood" enters into the tissues during the "assimilation time" of the liver (predominantly 11 PM to 6 AM), i.e. in the time of the glycogen and protein storage (2, 4, 7). Breakfast and dinner support the base floods during the day, whereby between meals short (approx. 2 hour) base low floods arise.
The liver rhythm is thus involved in controlling the hunger feeling and is even controlled from the hypothalamic Master Clock by the suprachiasmatic nucleus. Like all other cells it also has non-visual, photon-perceived "clock proteins" available, which feedback with the clock proteins of the liver cells. In regard to the Master Clock, changes in the environment, above all lighting conditions, but also temperature, behavior and nutrition are synchronized by the body cells (5). "The liver rhythm represents a '24 hour sine wave' for which the alimentary effects cause at most 'overtones'; like a clock can go faster or slower, and also like there are morning and evening people" (4). With a longer stay in a latitude [a part of the world] with for example opposite lighting conditions the circadian rhythm is gradually adjusted to it (4).
Rhythmic base floods are necessary because the NaHCO3, besides occurring in surplus in the ECM, can further dissolve and neutralize all the collagen fibers sticking to the acidic cell waste products (slag), supported by the buffer systems dissolved in the water domains of the PG/GAG's. The slag is delivered into the circulation, "assimilated" by the liver, modified for usual elimination with the urine, and secreted through the kidneys for recovery of the sodium ions. Besides, surplus sodium is secreted with the base flood, whereby the urine becomes basic or at least however neutral (4, 6, 7).
In contrast, the base low flood during the nocturnal assimilation liver phase leads to concurrent glycogen storage for "driving out" cellular by-products into the ECM where they are neutralized by the available buffers and are secreted after delivery into the blood directly over the kidneys under maximum sodium recovery (for regeneration of the buffers). As opposed to the daily urine, the nightly urine is thereby acid (4, 6, 7). Therefore it is an acid flood only in the urine, in the organism it corresponds to its base low flood (4). Acid urine represents a decreased alkali reserve in the ECM of the tissue, but no free acids. Practically, base floods and base low floods can best be measured from the urine pH (4).
Clogging up the ECM with Waste Products
Many living conditions, e.g. base-poor nutrition ("fast and junk foods") as well as diseases, especially chronic, lead to an increased sympathetic activity with increased inflammation expectancy and latent acidosis. Inflammatory mediators released by the macrophages and the granulocytes, above all the cytokine TNF- alpha, IL-1, and IL-6, lead to an increased proteolytic and hydrolytic enzyme activity in the ECM, supported on the side of the liver among other things by increased production of acute phase proteins, which further strengthens the pro- inflammatory reaction (1, 2, 4). The increasingly accumulating acidic metabolic products increasingly exhaust the buffer reserves so that they cannot sufficiently regenerate with base floods. Under these conditions almost complete back absorption of base equivalents by the kidneys is necessary revealing no more acid-base flooding in the urine, the urine is acid (4, 6, 7). For the ECM this means that the circadian rhythm absorption, storage and delivery are disturbed by the metabolic products. Since the replacement of collagen and PG/GAG's are fixed, increasingly accumulating acid molecules and their neutralization by alkali buffers can no longer sufficiently take place. Now the ECM begins to clog up under the picture of a latent acidosis. In the final analysis the ECM components are no longer bindable and also insufficient bufferable acids are shifted into the blood (e.g. ketonic acid in diabetics), where they then load the buffer capacities of the blood (4).
The tensegrity of the ECM is likewise made worse by which tension sensitive genes in the connective tissue cells are activated. This stimulates among other things macrophages for further formation of pro-inflammatory cytokine and fibroblasts through inadequate synthesis of ECM components – like too strongly acid-bound collagen and poorly connected PG/GAG's. "Inadequate" is called "situation-suitable" since the ECM synthesis occurs without distinction of "good and bad" (2). Thus the functioning of the ECM as a molecular sieve and actual regulator of the cell metabolism worsens. Consequently a variety of vegetative, functional and psychic symptoms develop without clear references to their causes (1, 4).
Therapeutic Possibilities
The clinical picture of "latent acidosis" corresponds conspicuously with syndromes which are strongly determined from individual conditions and are not caused tangibly, like chronic fatigue syndrome, depressive upset, visceral hyperalgesia, fibromyalgia, multiple chemical sensitivity, dysmenorrhea, post traumatic stress syndrome and obsessive-compulsive disorders (1, 4). For the general practitioner, these patients represent a considerable, above all time related, challenge in particular because he cannot rest on reliable diagnostic criteria. In principle, all causally understandable chronic diseases are also accompanied by a latent acidosis ("accompanying acidosis") (2, 4).
Causes of a latent acidosis are pathological acid formation in the organism and/or deficiency of base supply (4). To examine a latent acidosis is not usually well known or is neglected, although for example already a simple test of the urine pH by means of pH paper can give important references .
Even if the treatment of the basic disease is the focus of attention, do not on any account forget to include with it an anti-acidic treatment (2, 3). Because no therapy produces basic valences per se, they must be supplied exogenously by fixed bases (NaHCO3) directly and/or by whole foods. Exercise is also necessary with this, so carbon dioxide developed from NaHCO3 and HCl can be better breathed out (3). Stress reduction is likewise necessary for the reduction of the pro-inflammatory situation in the organism (1, 2). The stronger an acidosis is and the longer it already existed, the less available base still exists, and accordingly the base supply must be higher. On the other hand whether a "changing" takes place can be easily seen from the daily pH profile of the urine.
 An exclusive article for Members
An exclusive article for Members
From THE BRIDGE Newsletter of OIRF
Published September 15, 2007
From an article in Ärztezeitschrift für Naturheilverfahren
und Regulationsmedizin ◊ Volume 46, May 2005
Machine Translation by SYSTRAN, Lernout & Hauspie, LogoMedia & Promt
Translation & redaction by: Carolyn L. Winsor, OIRF
© Copyright 2005, Prof. Dr. Hartmut Heine, Neuhausen, Germany

Footnotes:
◊ This article is a lecture presented by Prof. Dr. Heine at the Viennese symposium “Acid-Base Cloggin Up” (25-26.02.2005) to honor of the 80th birthday of Prof. Dr. Dr. h.c. Alois Stacher.
◊◊ Translator’s note: “The word ‘tensegrity’ is an invention: a contraction of ‘tensional integrity.’ Tensegrity describes a structural-relationship principle in which structural shape is guaranteed by the finitely closed, comprehensively continuous, tensional behaviors of the system and not by the discontinuous and exclusively local compressional member behaviors. Tensegrity provides the ability to yield increasingly without ultimately breaking or coming asunder” – Richard Buckminster Fuller (excerpt from Synergetics, p. 372.)
Translation of diagram terms
Cortex = cortex
Basales Vorderhirnbündel = basal forebrain bundle
Zirkadian-rhythmus = circadian rhythm
cholinerge = cholinergic
adrenerge = adrenergic
dopaminerge = dopaminergic
serotoninerge = serotoninergic
System = system
Nichtvisuelle Photosens. = non-visual photosensitivity
Zirbeldrüse = pineal gland
Retina = retina
Ncl. solitarius = solitary nucleus
Ncl. coeruleus = nucleus caeruleus
Sättigung basogen = saturated basogenic
“Wiederholung” azidogen = “repeated“ acidogenic
Hirnstamm = brain stem
Retino-hypothal. Bündel = retino-hypothalmic bundle
Nucl. suprachiasmatis = nucleus suprachiasmaticus
Hypothalamus = hypothalamus
Nucl. arcuatus = arcuate nucleus
Appetitkontrolle = appetite control
HHN-Achse = hypothalamus-hypophysial-adrenal axis
Immunzellen = immune cells
Vagus (Parasympatikus) Sympathikus = vagus (parasympathic) sympathic
Stressoren = stressors
Magen = stomach
Leber = liver
Niere = kidney
Kochsalzkerislauf = sodium chloride (common salt) cycle
Matrix = matrix
latente Azidose = latent acidosis
Hypophysen = hypophysis
Nebennieren = adrenal
Säure-Basen Fluten = acid-base flooding
Zentrale Bedeutung des Kochsalzkerislaufes im zirkadianrhythmischen Säure-Basen Fluten des Körpersn = Central Importance of the Sodium Chloride Cycle in the Circadian Rhythms Acid-Base Flooding of the Body
Literature
- Berg PA. Neuroimmunologische Aspekte funktioneller somatischer Syndrome. Dtsch Med Wochenschr 2005; 130: 107-113
- Heine H. Grundregulation – eine Synthese medizinischen Denkens. Dt Ztschr f Akup 2004; 47: 7-19
- Korner J, Leibel RL. To eat or not to eat? – how the gut talks to the brain. N Engl J Med 2003; 349: 926-928
- Sander FE Der Säure-Basen-Haushalt des menschlichen Organismus. 2. Auf!. Stuttgart: Hippokrates Verlag, 1985
- Schwartz MW, Porte D Jr. Diabetes, obesity, and the brain. Science 2005; 307: 375-389
- Worlitschek M. Die Praxis des Säure-Basen-Haushaltes. 5. Aufl. Stuttgart: Haug, 2003
- Zander R. Physiologie und Klinik des extrazellulären Bikarbonat-Pools: Plädoyer für einen bewussten Umgang mit HCO3. Infusionstherapie, Transfusionsmedizin 1993; 20: 217-235
- Zilles K, Rehkämper G. Funktionelle Neuroanatomie. Berlin: Springer Verlag, 1993
")
