
This thesis applies specifically to the action of the SNS upon the cardio-vascular system. This thesis is for your understanding. It is not meant to be used as an erudite scientific dissertation.
Acknowledgment: I acknowledge that the information I am giving you is the lifelong research and work of Dr. med. Peter Hain, a German cardiologist currently Medical Director of the Neuen Wicker Kliniken in Bad Nauheim, Germany.
| Abbreviation | |
|---|---|
| leads to / affects | |
| ANS | Autonomic Nervous System controls the involuntary, emotional aspect of our actions. It consists of two parts – SNS and PSNS. |
| SNS | Sympathetic Nervous System is responsible for all the nervous system and hormonal aspects of the flight/fright/fight responses. |
| PSNS | Parasympathetic Nervous System is responsible for all the nervous system and hormonal aspects of the relaxation/ digestive responses. |
| CVS | Heart, coronary arteries, circulation and brain circulation. |
| GIT | Gastro-Intestinal Tract, digestive processes |
| BP | Blood Pressure |
| Myocardium | Heart muscle |
| CFS | Chronic Fatigue Syndrome |
| CCF | Chronic Congestive Failure |
| GUT | Genito-Urinary System |
| EMR | Electromagnetic radiations, including electrical appliances, mobile phones, micro-wave oven cooking |
The Cause of the Problem
Stress means any change imposed on your organism
![]() Stimulates the ANS
Stimulates the ANS
![]()

Dys-stress
Any distress including:
Emotions, Inflammation, Allergies, Diseases, Nutrition, Intoxication, Pollution,
Excessive/Inappropriate Exercise, EMR exposure, watching TV, or driving your car.
Even talking can be a distress.
![]() Chronic over-stimulation of the SNS
Chronic over-stimulation of the SNS
![]() Increased tension in the myocardium – the muscle of the heart.
Increased tension in the myocardium – the muscle of the heart.
![]() Consequences in:
Consequences in:
– the heart muscle
– the coronary arterial circulation
– the arterial output
– the venous return.
What Happens
Stimulation of the SNS
![]() triggers the neurological and hormonal changes needed to deal with
triggers the neurological and hormonal changes needed to deal with
FLIGHT, FRIGHT, FIGHT response to environmental stresses.
In the acute, short term situation, this leads to an increase in heart rate, an increase in cardiac output, and an escape or solution to the stressor.
In the chronic state, this stimulation goes on and on and on and on and on . . . A whole new counter-productive situation arises.
Chronic, on-going low grade stressors
![]() Chronic persistent over-stimulation of SNS
Chronic persistent over-stimulation of SNS
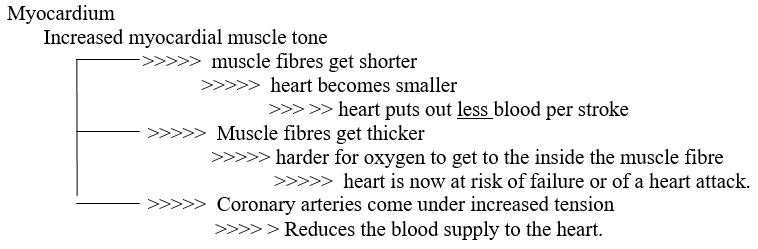
![]() Increased myocardial muscle tone
Increased myocardial muscle tone
![]() Reduced heart out put per beat
Reduced heart out put per beat
![]() Increased heart rate
Increased heart rate
Heart works harder, palpitations, arrhythmias.
Increased resting pulse.
Heart has less time to relax between beats.
![]() Increased pressure on the peripheral circulation –> eventually high blood pressure.
Increased pressure on the peripheral circulation –> eventually high blood pressure.
Consequence: The heart becomes inefficient and insufficient across all functions of the body. Not just when we need it more (eg. during exercise / work / life), but also at rest, in bed. And more importantly when we push our bodies to the limit during sports and other serious events in our lives.
The heart is not broken. It is insufficient.
This means common investigations like GPs, heart specialists, blood tests, ECG, radio-thallium exercise stress tests and the gold standard for heart function, coronary angiograms, will not be able to diagnose the problem early, when it really matters most!
Heart Insufficiency
Heart insufficiency
![]() A relative decrease in heart output –> Reduced blood supply to the rest of the body
A relative decrease in heart output –> Reduced blood supply to the rest of the body
![]() Increased pulse rate –> Increased resting pulse rate, palpitations, arrhythmias, CFS
Increased pulse rate –> Increased resting pulse rate, palpitations, arrhythmias, CFS
![]()
This now leads to a host of symptoms including:
- Reduced stamina, unreasonable fatigue & tiredness, CFS,
- Shortness of breath on mild exertion
- CCF
- Risk of sudden unexpected death. Heart attacks. Strokes.
- (Maybe even SIDS)
The odd and very tragic thing about this scenario is that,
- the fitter the body,
- the greater risk of developing this condition and
- the greater the risk of early and serious consequences.
All of which have been totally unpredictable.
How the Body Deals With the Difficulty
The Body copes by increasing the blood volume through two mechanisms.
a) By creating generalised tension in the blood vessels. This means the same amount of blood occupies a smaller volume inside the blood vessels.
b) By causing fluid retention.
Heart Insufficiency
![]() Increases tension in blood vessels
Increases tension in blood vessels
![]() Increased or obvious high BP
Increased or obvious high BP
![]() Reduces the circulation to the kidneys
Reduces the circulation to the kidneys
![]() Fluid retention.
Fluid retention.

The body compensates for this heart insufficiency by increasing the tone in the SNS. This is what caused the problem in the first place. The whole problem now begins to be self perpetuating.
The Effects of the Increased Blood Volume
The increase in blood volume has different effects when standing and when lying or sleeping.
Standing:
The excess volume, under the action of gravity, accumulates in the legs where it causes
- tired, restless legs,
- swollen ankles
- veins
- congestion in the abdomen with gut symptoms.
Lying:
The extra blood is now free to enter the general circulation. The heart is now under the full influence of the extra blood volume. The heart has to work harder at the very time you want to rest. This increases the SNS tone.
This results in
- rapid heart beat,
- palpitations,
- disturbed sleep.
- Wakefulness.
- being wide awake when you need to sleep.
- waking tired and unrested.
- inability to sleep on your left side.
The body does give us warning signs, but they are not clearly and obviously heart related.
The increase in venous volume means that there is a difference between the concentration of blood in the arteries compared with that in the veins. A simple blood test can be very diagnostic. But the accuracy of the test depends on how the blood is collected. This is why this blood test is collected and carried out by my trained staff at the WHWI.
Another test that may be carried out is an ECG. But this one is done in two stages.
The first ECG is carried out with the patient lying flat on their back.
The second ECG is carried out with the patient lying on their back, but with their feet elevated.
The two ECGs will be compared to see if there are any differences.
An ultra-sound taken of the heart during contraction and during relaxation may reveal how much tension there is the heart. Other cardiac output investigations are rather too sophisticated for our purpose.
A Summary of the Normal Condition
Normal and Healthy Situation
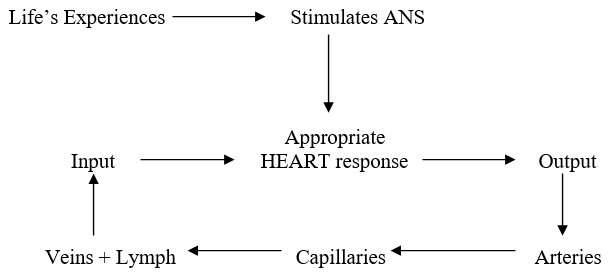
Heart Input is equal to heart output.
A Summary of the Acute Situation of Stress
Acute Stress / Dys-stress / Change
![]() Increased SNS tone
Increased SNS tone
![]() Heart is stimulated.
Heart is stimulated.
Increased heart tone. Increased pulse rate. Reduced heart output per beat.
Overall increase in heart output.
( The heart does not have to be efficient. It just has to get your skin out of there safely.)
![]() Increased arterial tone.
Increased arterial tone.
Increase in blood supply to survival sustaining organs.
Decrease in blood supply to non-essential organs.
![]() Increased leaking of fluid into the lymph.
Increased leaking of fluid into the lymph.
![]() Decreased venous return to the heart.
Decreased venous return to the heart.
A Summary of the Chronic Situation
Chronic Dys-stress:
![]() Increased SNS tone
Increased SNS tone
![]() Heart is stimulated non-stop.
Heart is stimulated non-stop.
Increased heart tone. Increased pulse rate. Reduced heart output per beat.
Decrease in circulation to the heart. Overall decrease in heart output.
![]() Increased arterial tone.
Increased arterial tone.
Increase in blood supply to survival sustaining organs.
Decrease in blood supply to non-essential organs. These organs begin to suffer.
Increase in blood pressure places stress on the heart, blood vessels, kidneys and brain.
![]() Increased leaking of lymph into tissues causes swelling, oedema and inflammation.
Increased leaking of lymph into tissues causes swelling, oedema and inflammation.
![]() Increased pooling of blood in the veins.
Increased pooling of blood in the veins.
![]() Heart is unable to adequately “suck blood out” of the venous input side of the vascular system.
Heart is unable to adequately “suck blood out” of the venous input side of the vascular system.
![]() Heart Insufficiency.
Heart Insufficiency.
Another consequence of Heart Insufficiency is that the lowered heart output means the blood supply to the entire body is reduced, reducing the net oxygenation of the body tissues.
This means that the entire body metabolism becomes compromised, showing up as a plethora of symptoms that seemingly have no relationship to one another. So the patient is told that “the illness is all in the mind”, that there is “no cause for the symptoms”.
Cardiologists talk about the heart efficiency, as the heart/cardiac output being a percentage of what is called “normal”. The problem in Heart Insufficiency is that the heart/cardiac is ALREADY reduced significantly. So discussing the percentage of an already reduced heart/cardiac output, as if heart insufficiency did not exist, is completely misleading and potentially harmful. Harmful because it lulls everyone by not understanding what is really going on.
The ONLY true measure of heart/cardiac efficiency is to measure the ACTUAL heart/cardiac output.
The relative hypoxia (lack of oxygen to the tissues) stimulates the breathing centre in the brain stem, which in turn induces hyper-ventilation.
Hyper-ventilation washes carbon dioxide out of the blood causing a Respiratory Alkalosis and a Metabolic Acidosis.
The alkalosis binds calcium and magnesium ions that triggers muscle spasm. Patients now complain of rheumatic aches and pains, joint damage, myo-fascial trigger points, CFS.
The hyper-ventilation induces an anxiety state, which may include panic attacks, obsessive and compulsive behaviour patterns.
The risk here is that the patient presents in an acidic condition, (NB: the BE-T-A does not test arterial blood, so it will not pick this up), and will be given alkalinizers which will make the whole condition even worse.
Heart Insufficiency also triggers the brain stem cough centres, leading to a particularly intractable cough. This becomes a real problem when the patient is also taking ACE-inhibitors.
The Treatment
The treatment is on three levels:
- Find the cause and fix it.
- Treat the emotional triggers that activate the SNS.
Ultimately, no treatment will really work unless we correct the self perpetuating condition.
This is the excess blood volume.
The way to do this is to reduce the excessive venous volume.
We do this by taking some blood. The exact volume will depend on the difference in the venous/arterial hematocrit levels, and how you feel while the procedure is taking place.
The amount of blood that we take is about the same that a woman would loose during her menses. Any more could trigger the SNS and be completely counter-productive. So giving blood to the Blood Bank may simply be too much.
Interestingly: If you do not have this condition, then you can donate blood to the blood bank with no ill effects. But if you do have this condition, donating blood may trigger an increase in the SNS tone, which could have un-toward effects.
The reduction in venous blood volume removes the stimulation to the SNS and triggers a relaxation response, which opens up the heart, and the circulation. This is the very response we are looking for.
How often might you need such a treatment?
Initially once a week until you are feeling really well. Then once a month for about six to twelve months, depending on your blood test results.
You may need to have your blood tests carried out at least once a year for a long time.
 An exclusive article for Affiliates
An exclusive article for Affiliates
From THE BRIDGE Newsletter of OIRF
Published December 8, 2005
© Copyright 2005, Dr. Zenon Gruba, Victoria Australia

")
