
Long-Term Inhibition of the Immune
System by Corona Vaccines, Part I
The consequences of Corona vaccinations can be drastic, as more and more studies show: vaccinated people have a greater risk of getting sick from Corona, and to die from it, than the unvaccinated. They are also prone to a persistent weakness of the immune system and to the development of cancer. Scientific findings can now conclusively explain how these fatal effects occur.
In general, with the progress of a vaccination campaign the incidence of the infectious disease against which you are vaccinated is expected to decrease as the rising vaccination levels of the population increases. With the new Corona vaccines, exactly the opposite is the case.
Epidemiological Warning Signals
A largescale epidemiological study from Harvard University states1: The more people who are vaccinated against Corona, the more Corona cases are registered. This correlation not only concerns case numbers in general, but specifically also Corona associated death cases (died of/with Corona2).
Figures from Scotland3 have proven for months that vaccinated people more frequently land in the hospital and in intensive care with Covid-19 in comparison with unvaccinated people, and also in the end more frequently pass away of/with the infection. Studies from England and Scandinavia also prove a “negative effectiveness” of the vaccination, especially against Omicron and after multiple vaccinations (“Boosters”).4, 5 However, terms such as “Booster” and “Negative Effectiveness” are euphemisms of the first order: What is actually expressed here is a lack of effectiveness and/or a harmful effect rather than a protective effect. If a vaccination increases the likelihood of becoming ill and of dying of exactly the infectious illness against which was vaccinated – then something seems to be wrong with the effect of this vaccination on the immune system. Rather these findings represent a warning signal that undesirable immunological effects are occurring here, and the background, mechanism and consequences must be urgently investigated. However this is exactly what the licencing and supervisory authorities stubbornly refuse. Besides, these “field experiences” are certainly not the only indications of serious problems.
What is actually expressed here is a lack of effectiveness and/or a harmful effect rather than a protective effect.
The Renaissance of Shingles
In people who have undergone a Corona vaccination recurrences of viral infections occur increasingly frequently: latent viruses dormant in the body for a long time are reactivated and there is a flaring up of infections that have actually been borne for many years and decades. The classic in this regard is shingles (herpes zoster),6, 7 however analogously this effect is also observed with EBV (Epstein-Barr virus, mononucleosis), CMV (cytomegaly virus), hepatitis viruses,8 Lyme borreliosis and other pathogens. An intact immune system is well finished with such dormant pathogens and leaves them with no chance. However, if the immune system is sufficiently weakened or hindered, they reach the head water, increase once more and cause further associated complaints and clinical phenomena. Primarily shingles appears after the Corona vaccination so frequently that meanwhile Pfizer/Biontech works on an RNA vaccine against zoster viruses to also cover this (self-created) business segment. Reactivation mechanisms of this kind are nothing new medically. These phenomena occur within the scope of various medical interventions as an undesirable side effect – for example as a consequence of an immune suppression with autoimmune illnesses or chemotherapy for cancer. In such a context, the induced defense weakness is consciously accepted because the overall benefit outweighs the harmful effect. On the other hand that such a cost-benefit calculation is also valid for a protective vaccination may be doubtful. Also here the warning signals in the sense of immune damage are not followed up. Something with the immune system of vaccinated people seems to be wrong. In this case what would be more detailed than to cast a first look into the licencing studies, to look which immunological parameters were raised and proven here within the scope of the development of the new gene therapeutic immune intervention?
Immunological Findings from the Licencing Studies
Thanks to telescoping and extremely lax performance targets from the supervisory authorities, reading the licencing studies from all the manufacturers proves to be extremely sobering. Sometimes a real placebo was dispensed with (AstraZeneca was tested against meningococcal vaccine, Valneva against AstraZeneca), and sometimes completely on laboratory parameters (Moderna Phase 2/39). When the laboratory parameters were raised, they were then extremely superficial – the checked values correspond to a normal blood count with the family doctor and are in no way suitable to map immunological safety risks of an experimental gene therapy. General inflammation markers (ESR, CRP), liver and kidney values as well as a blood count, nothing more.10 Besides, it is known from the development of former vaccines that considerable immunological problems can appear – especially as concerns vector vaccines,11 vaccines against corona viruses12 and active ingredients based on nanoparticles.13 Then it should have been successful to develop a vector vaccine or a vaccine based on nanoparticles against Corona virus within months. Something which has still never succeeded to date and after decades of research. The licencing studies reveal how this miracle was possible: relevant potential risks were consequently not, or only insufficiently, investigated – which naturally makes failure unlikely. Manufacturers and authorities essentially fixated on a single surrogate marker to assess the success or failure of the vaccine: the quantitative appearance of SARS-CoV-2 spike antibodies. Meanwhile however, thanks to the courageous work of independent researchers and doctors we know a great deal about the profound consequences of gene vaccinations on our immune system. The knowledge is astounding, further questions are raised and leave nothing good foreseen in perspective. It is not without reason that people talk about V-AIDS (Vaccine-AIDS), in order to describe the collateral damage of the Corona vaccinations. To avoid misunderstandings: V-AIDS does not mean infection with the HIV virus. AIDS simply stands for Acquired Immune Deficiency Syndrome, in other words acquired immunodeficiency syndrome, thus an acquired massive insufficiency of the immune system. In this case not from a virus (HIV) but rather from a vaccination (vaccine).
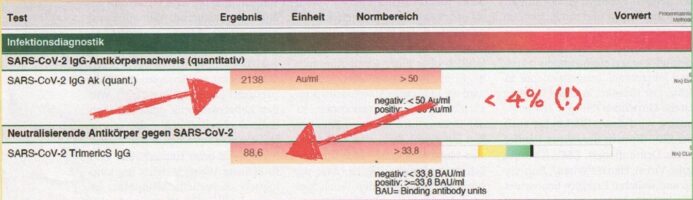 Figure 1: Antibody profile of a triply vaccinated person: neutralizing antibodies constitute
Figure 1: Antibody profile of a triply vaccinated person: neutralizing antibodies constitute
less than 4 percent – the Paul Ehrlich Institute (PEI) ignores these findings:
Laboratory Biovis; © F. Schilling.
More ADE: Higher Virus Load, Fewer Defensive Cells
A few viruses are able to trigger the production of dysfunctional antibodies, which instead of fighting pathogens, they accelerate the increase while they destroy the immune system at the same time. Previous vaccine developments based on vectors (dengue fever11) or against corona viruses12 (SARS, MERS) failed precisely because they triggered the formation of infection-enhancing antibodies (ADE, “antibody-dependent enhancement”). These enable the virus to penetrate our scavenger cells (monocytes, dendritic cells) unscathed, to multiply there explosively and to destroy the affected defense cells. The result: The virus load increases rapidly in the case of an infection while the number of defense cells drops dramatically – a fatal combination that leads to more severe, complicated and deadlier courses. From previous research results it was known that this phenomenon with vaccinations against corona viruses must be calculated with a frequency of 1:15. It was also known that the spike protein of SARS-CoV-2 is also highly likely to be able to trigger ADE based on its molecular characteristics.14 During the licencing phase, the manufacturers investigated the situation either not at all or with only a few laboratory animals (maximum: 12). Not unexpectedly there was no indication of ADE. Meanwhile, researchers independently made up for these investigations with several hundred laboratory animals. Their results: the Corona vaccination caused ADE at 6 percent in laboratory animals.15 In the absence of representative cohort studies we must transfer this ratio to vaccinated people for the time being. Meanwhile laboratory investigations prove that many vaccinated people show an extremely critical antibody status. Not only the total number of antibodies decreases very quickly after the vaccination (which is why after only a few months a “Booster” is recommended) – but rather it shows that on a large part the available antibodies posses no neutralizing effect. Figure 1 shows an example of the values of the boosted patient in which the neutralizing antibodies make up less than 4 percent(!) of the total SARS-CoV-2 antibodies. The urgent question arises, what are the remaining 96% of the antibodies occupied with – with T-Regs?
More T-Regs: Less Immune Activity Regarding Cancer and Infection
T-Reg (regulatory T-cells, synonymously T-suppressor cells) are special T-lymphocytes whose task consists of monitoring the rest of the immune system. They prevent uncontrolled, excessive immune activity (e.g. allergies, autoimmune reactions, hyperinflammation) and are carriers of immune tolerance. Insufficient activity of these cells can have serious consequences – conversely an increased activity leads to significant defense deficits. Overstimulated T-reg can figuratively be compared to a car that drives with the handbrake firmly applied. With cancer illnesses, overzealous T-reg regularly constitutes a problem, because they guard the cancer cells from the rest of the immune system and inhibit these at various levels.16 The higher the T-reg the more unfavorable the prognosis. This is also valid for defense from pathogens – especially viruses. Patients with severe Covid courses frequently exhibit increased T-reg.17 For a long time is has been known that repeated vaccination against one and the same opponent leads to the formation of T-reg.18 Result: in fact it develops plentiful antibodies, however thanks to the inhibition from the T-reg no effective protection is guaranteed. Post-mortem examination of vaccinated people who died of Covid showed extremely high antibody levels – and at the same time showed massive virus infestations in all possible organs and tissues.19 The firmly applied handbrake in action. With allergies you knowingly make use of this functional principle within the framework of hypo-sensitization: the repeated injection of allergens leads to increased formation of T-reg, the immune system is increasingly more tolerant of the antigen, the allergic inflammatory reaction fades away. Meanwhile even the EMA [European Medicines Agency] expresses concerns whether the many times repeated vaccination against Corona could not lead to an “excessive demand” on the immune system.20 Cytokine measurements and T-reg levels in vaccinated people, their increased infection rates in comparison with unvaccinated people, autopsy findings and the massively increasing number of “vaccine breakthroughs” (especially with severe cases) clearly establishes an indication of stimulation of T-reg through booster vaccination. Simply stated: the more often people are vaccinated against Corona, the more tolerant the immune system becomes to SARS-CoV-2. The problem is that the tightening of the handbrake also affects other areas, not “only” Corona – especially with protection from cancer as well as infection from new ones, like a virus unknown to the body until then. In both areas, an increase in the number of diseases is to be expected in the medium term.21
Meanwhile even the EMA expresses concerns whether the many times repeated vaccination against Corona could not lead to an “excessive demand” on the immune system.20
Fewer Interferons: Less Protection from Viruses and Cancer
With interferons it is about multifunctional signaling molecules of the immune system. On the one hand they serve the communication and stimulation within the immune system. On the other hand they are veritable weapons to destroy viruses, infected cells and cancer cells. In case of a viral infection interferons can already slow down the multiplication of the virus very early, even before specialized defense cells can intervene in the occurrence. Therefore they furnish our organism time to build up an adequate resistance and prevent an explosion of the virus load. Thus the risk of severe and highly inflammatory courses is reduced. Yes, it is exactly the latter that can potentially make Covid-19 a fatal disease. In cancer cells interferon triggers apoptosis, the controlled suicide of the malignant cell. They are thus one of the most important primary protective mechanisms against cancer. Interferons are also used in oncology as immuno-therapeutics to fight the tumor and prevent relapses. Conversely: Interferon levels in a cancer patient are low, this is regularly accompanied by an unfavorable prognosis.22 During and after a natural infection with SARS-CoV-2 interferon levels build up in the organism. Conversely the Corona vaccination leads to a dramatic decrease in interferon.23 Meanwhile this has also been explained why: particularly RNA vaccines lead to a profound, genetic reprogramming of our defense cells. Genes which are responsible for interferon formation are switched off, the same is valid for the genes of the interferon receptors.24 Result: fewer messenger substances reach fewer receptors. This leads to a massive inhibition of large parts of the immune system. Through quadruplex and prion formation this trend is again clearly aggravated.25 Because this concerns a genetic effect, because the RNA vaccine persists in the body for at least months26 and because it can be transcribed into the DNA,27 the immunological damage is unfortunately very long lasting.
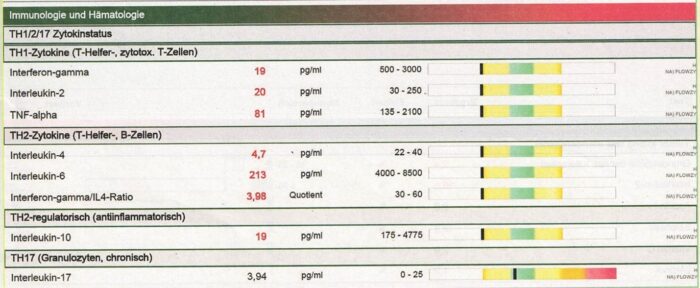 Figure 2: Cytokine profile of a “boostered” patient: No provable
Figure 2: Cytokine profile of a “boostered” patient: No provable
significant activity of the helper cells, Laboratory Biovis: © F. Schilling.
Killer Cells and Helper Cells Hardly Efficient
Added to the problems described so far, there is also the aspect of functional exhaustion. This primarily pertains to two cell types of the immune system: natural killer cells (NK-cells) and T-helper cells. Let us think of the immune system as an army. Then the T-helper cells correspond to the general staff, and the NK-cells to the elite combat troops. It makes sense that the chances of winning a battle, let alone a war, are minimal if the general staff is unreachable and does not give orders. The same thing is valid in the case that the storm troopers refuse the attack order. Exactly this mixed situation frequently appears in vaccinated people. By measuring the cytokines (messenger substances of the immune system) you can determine the communication of the immune system as well as its activity derived from this. If you start such an eavesdropping with vaccinated people, especially boostered, the result is frequently total silence. An example here is the Th1/Th2 cytokine profile quoted in Figure 2: neither the cellular (Th1 killer cells) nor the humoral (Th2 antibody) defense show an adequate basal activity in the profile. Such a configured immune system is in no way able to provide an adequate defense in an emergency. On the other hand classical emergency situations are infections (especially with new unknown pathogens) as well as elimination of cancer cells in the body. About the willingness of the natural killer cells to perform, it is frequently similarly poorly ordered. It can be determined by a so-called cytotoxicity test: you isolate NK-cells from a blood sample of a test person and cultivate it in the laboratory together with cancer cells. Subsequently it can be determined how many of the cancer cells can be destroyed by the natural killer cells. An extremely realistic emergency case scenario. Depending on the laboratory the reference values will be somewhat different, nevertheless at least 20 percent of the cancer cells should be destroyed within the scope of the cell estimates. However with vaccinated people the elimination rates often lie in the single digit range, in some instances under 5 percent. Also, like the example shown in Figure 3, the killer cells of the patient can only destroy 2.4 percent of the cancer cells. This corresponds to a functional loss of 90 percent.28 This will not cause acute complaints where the medium- and long-term risks of a cancer illness are concerned. However, here you should not indulge in any more illusions.
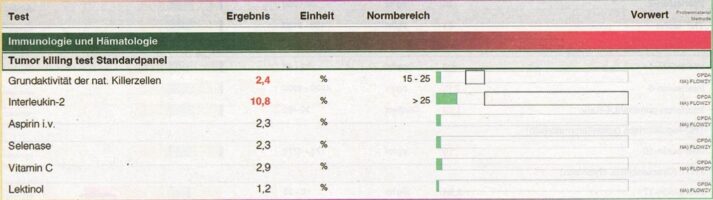 Figure 3: NK-activity after booster vaccination: Laboratory Biovis; © F. Schilling.
Figure 3: NK-activity after booster vaccination: Laboratory Biovis; © F. Schilling.
Conclusion and Outlook
New findings of possible risks and harmful effects of corona vaccinations are published almost daily. The list of potential and already proven problems is getting longer and longer. To date, what is concerning with the known damages to the immune system is that a magnitude has been reached which absolutely justifies the use of the term V-AIDS. While at the moment the acute complications and damages are still in the foreground (autoimmune diseases, clot formation, heart muscle inflammation, infarctions) we must assume that the induced immunosuppression shows the greatest damage potential in the medium- to long-term. The next pandemic virus, perhaps already even the next SARS-CoV-2 variant, will strike those affected by V-AIDS with all its force. The number of new cancer illnesses will climb significantly in the next years, and the first trends are already emerging here. Established colleagues speak of “turbo-cancer” which is characterized by aggressive growth and increased resistance. Relapses (return of successfully treated cancer illnesses) increase in considerable extent. In 2021 (and thus since the introduction of the compulsory vaccination for its soldiers) the medical database of the US Department of Defence recorded a growth rate of 300 to 850 percent for cancer illnesses. Meanwhile this data was taken offline and was “reworked” to include previous years. If you take into consideration the fact that most physicians are not familiar with the described pathophysiological connections or the special examinations to make them visible, and if you furthermore take into consideration that until now we still simply lack the instrumentation to eliminate many of these problems, then it becomes clear that we are going towards difficult times. The perspective does not improve if you take a look at the current decision-makers and those responsible in politics; supervisory authorities and professional associations. The vaccination is officially considered to be virtually side effect free, and contrary statements (even when they are so well proven by studies, laboratory measurements and clinical documentation) are considered as malicious conspiracy theories. Critical voices are at best ignored, at worst the critics are removed from their positions, covered with lawsuits or exposed to character assassination campaigns. At this point to describe the learning curve for the system as flat is euphemistic. Fortunately worldwide, but also in this country, there are committed scientists and physicians who confront the challenges outlined here, who research, document, experiment and bit by bit develop solutions. My deeply felt thanks and respect are held for them at this time. Above all at this moment, I see my task as gathering this knowledge and making it available to as many people as possible.
 For this purpose I have published numerous videos, diagnostic protocols and therapy recommendations on my blog. This content is available free of charge at https://www.florianschillingscience.org/ A deepening and detailed processing of the various aspects is possible with the help of the books that have now been published. In the context of this article in particular the most recent one: “Post-Vakzin-Syndrom: Handbuch für Gaschädigte der Corona-Impfung” [Post Vaccine Syndrome: Manual for Victims of the Corona Vaccination.]
For this purpose I have published numerous videos, diagnostic protocols and therapy recommendations on my blog. This content is available free of charge at https://www.florianschillingscience.org/ A deepening and detailed processing of the various aspects is possible with the help of the books that have now been published. In the context of this article in particular the most recent one: “Post-Vakzin-Syndrom: Handbuch für Gaschädigte der Corona-Impfung” [Post Vaccine Syndrome: Manual for Victims of the Corona Vaccination.]
In the next issue, Florian Schilling will write about how the harmful effects of vaccination can be countered therapeutically.

An Exclusive Translated Article for P2P Supporters
From the Monthly Publications of P2P
Published November 2022
From an article in Raum&Zeit, Volume 41, Nr. 238, July/August 2022
Machine Translation by SYSTRAN, Lernout & Hauspie, LogoMedia & Promt
Translation & redaction by: Carolyn L. Winsor, P2P Consulting
© Copyright 2022, R&Z, Florian Schilling, Munich area, Germany
Florian Schilling: “Post-Vakzin-Syndrom: Handbuch für Geschädigte der Corona-Impfung”, tredition, 2022, 45,- €, ISBN: 978-3347544635

Footnotes
- Subramanian, S. V., Kumar, A. (2021): „Increases in COVID-19 are unrelated to levels of vaccination across 68 countries and 2947 counties in the United States. European journal of epidemiology, 1-4″
- Fenton, N., Nell M. (2021): “No fancy statistics: a simple plot of vaccination rate against Covid death rate for all countries in the world: Probability and Risk [Online], http://probabilityandlaw.blogspot.com/2022/01/no-fancy-statistics-simply-plot-of.html (Accessed 19.04.2022)”
- Scotland, P. H. (2022): COVID-19 statistical report – 16 February 2022, https://publichealthscotland.scot/publications/covid-19-statistical-report/covid-19-statistical-report-16-february-2022/
- Hansen, C. H., Schelde, A. B., et al. (2021a): „Vaccine effectiveness against SARS-CoV-2 infection with the Omicron or Delta variants following a two-dose or booster BNT162b2 or mRNA-1273 vaccination series: A Danish cohort study. medRxiv”
- Agency, U. H. (2022): „COVID-19 vaccine surveillance report Week 2′, https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1047814/Vaccine-surveillance-report-week-2-2022.pdf
- Wan, E. Y. F., Chui, C. S. L, et al. (2022): „Herpes zoster related hospitalization after inactivated (CoronaVac) and mRNA. (BNT162b2) SARS-CoV-2 vaccination: A self-controlled case series and nested case-control study. The Lancet Regional Health – Western Pacific, 21″
- Van Dam, C. S., Lede, I., al. (2021): „Herpes zoster after COVID vaccination. Int J Infect Dis, 111, 169-171″
- Lensen, R., Netea, M. G., et al. (2021): „Hepatitis C virus reactivation following COVID-19 vaccination-A case report. International Medical Case Reports Journal, 14, 573″
- Baden, L. R., Sahly, H. M., et al. (2020):.„Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. New England Journal of Medicine, 384, 403-416″
- Polack, F. P., Thomas, S. 1, et al.: „Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. 383, 2603-2615″
- Halstead, S. B. (2018): „Which dengue vaccine approach is the most promising, and should we be concerned about enhanced disease after vaccination? Cold Spring Harbor perspectives in biology, 10, a030700″
- Eroshenko, N., Gill, T., et al. (2020): „Implications of antibody-dependent enhancement of infection for SARS-CoV-2 countermeasures. Nature Biotechnology, 38, 789-791″
- Dwivedi, R. (202/): „Research looks at inflammatory nature of lipid nanoparticle component in mRNA vaccines. @NewsMedical”
- Ricke, 0. (2021): ,Two Different Antibody-Dependent Enhancement (ADE) Risks for SARS-CoV-2 Antibodies. Frontiers in Immunology, 12, 443″
- Farshi, E. (2020): „Cytokine Storm Response to COVID-19 Vaccinations. J Cytokine Biol, 5, 2″
- Curiel, T. J. (2007): „Tregs and rethinking cancer immunotherapy. J Clin Invest, 117, 1167-74″
- Galvän-Pena, S., Leon, J., et al. (2021): „Profound Treg perturbations correlate with COVID-19 severity. Proceedings of the National Academy of Sciences, 118, e2111315118″
- Wang, S.-M., Tsai, M.-H., et al.: (2012): ”The regulatory T cells in anti-influenza antibody response post influenza vaccination. Human vaccines & Immunotherapeutics, 8, 1243-1249″
- Hansen, T., Titze, U., et al.: (2021b): „First case of postmortem study in a patient vaccinated against SARS-CoV-2. International journal of infectious diseases : IJID : official publication of the International Society for Infectious Diseases, 107, 172-175″
- EMA (2022), EMA says not enough evidence for a second COVID booster’, https://www.euractiv.com/section/coronavirus/news/ema-says-not-enough-evidence-for-a-second-covid-booster/
- Barth, S. D., Schulze, J. J., et al.: (2015): „Treg-Mediated Immune Tolerance and the Risk of Solid Cancers: Findings From EPIC-Heidelberg. JNCI: Journal of the National Cancer Institute, 107.”
- Marth, C., Fiegl, H., et al. (2004): „Interferon-ƴ expression is an independent prognostic factor in ovarian cancer. American Journal of Obstetrics and Gynecology, 191, 1598-1605.”
- lvanova, E. N., Devlin, J. C., et al. (2021): „SARS-CoV-2 mRNA vaccine elicits a potent adaptive immune response in the absence of IFN-mediated inflammation observed in COVID-19. medRxiv, 2021.04. 20.21255677″
- Liu, J., Wang, J., et al. (2021): „Comprehensive investigations revealed consistent pathophysiological alterations after vaccination with COVID-19 vaccines. Cell”
- Ibid
- Röltgen, , Nielsen, S. C. A., et al.: „Immune imprinting, breadth of variant recognition, and germinal center response in human SARS-CoV-2 infection and vaccination. Cell”
- Alden, M., Olofsson Falla, F., et al. (2022): „Intracellular Reverse Transcription of Pfizer BioNTech COVID-19 mRNA Vaccine BNT162b2 In Vitro in Human Liver Cell Line. Current Issues in Molecular Biology, 44, 1115-1126″
- Johnson, R. (2022): „DOD whistleblowers reveal data showing increases in medical conditions among service members; raise concerns about COVID-19 vaccine safety”, Available: https://www.ronjohnson.senate.gov/2022/2/sen-johnson-to-secretary-austin-has-dod-seen-an-increase-in-medical-diagnoses-among-military-personnel
")
