
Focal Point
Disturbance Fields and Foci
And Other Causes of Chronic Complaints
For Readers in a Hurry
An exact anamnesis of the chronological references, and knowledge of the phenomena connected with the disturbance field effect, are indispensable for disturbance field diagnostics. The evidence for the presence of a disturbance field is the successful treatment.
Disturbance fields are co-causes of the clinical picture for up to 30% of all patients with chronic or recurrent difficult to treat complaints. This is why the topic is of great importance and is differentially considered in the following article.
“ . . . and then I even cleared the scars.” I have often heard this said by seminar participants. My questions back [to them] regularly provoke astonishment: “Why cleared? You have treated the scar. How do you know whether they are disturbed? And if yes, what and how?” Apparently, it is taught in various therapeutic contexts that all scars should be cleared. Mind you, it is not a matter of symptomatically treating scars with unpleasant feelings or pain, or scars that itch or are swollen.
Scars should be cleared because scars can be disturbance fields and can trigger various symptoms that show no known functional connection to the disturbance field. Strictly speaking however, scars do not necessarily have to “disturb”.
Disturbance fields can disrupt the body’s autoregulation.
We struggle over and over again with a lack of conceptual clarity when it is an expression like “focus illness”, “disturbance field” and “clearance”. This lack of conceptual clarity necessarily leads to therapeutic uncertainty. There are many reasons for these uncertainties, lack of conceptual clarity and confusion.
The concepts between a focus illness, a focal toxicosis and a disturbance field must also be differentiated. Therefore, we would like to examine these concepts more exactly.
Focus illnesses from local bacterial foci have become very rare thanks to modern antibiotics and image-based procedures. We most likely find bacterial foci in tooth pockets which can result in heart illnesses, and bacterial metastases even into the joint cavity with immune deficient patients.
Focal toxicosis from foreign particles or toxic medications, such as previously after injections with mercury preparations, has become very rare. [Current] examples are symptoms from metal abrasion with hip prostheses or from leaking breast implants.
Foci and focal toxins can develop into disturbance fields. [Such] a connection does not necessarily exist. There are many disturbance fields that are not from either. With medical advances the bacterial and material burdens play a far lower role for disturbance field genesis in the tooth-jaw area than the mechanical stressors from orthodontics and prosthetics. With a mostly multifactorial disturbance field genesis, materials as a final factor could bring the system to the borderline. However, they are most rarely the main factor. Tooth redevelopments lead to a string of radical changes in the teeth, to occlusion problems and undetermined risks through new materials. If cranial-sacral therapy(4) helps in the mouth-tooth-jaw system, we would rather repeatedly offer this than encumber our patients with difficult to assess structural risks in the teeth.
Relationships of Scars and Disturbance Fields
Disturbance fields, and thus also disturbing scars, can confuse the body in all functions of its autoregulation. They disrupt with some serious consequences. Disturbing scars and other disturbance fields are defeated by our regularization physiology. If it was different, we could not functionally treat disturbance fields successfully. A clear and specific therapeutic intervention is vital(1) for a possible balance of a disturbance. Because of that, only one specific, clear and significant to the patient stimulus-effect will be therapeutic. Otherwise, the accidental tension and pressure, a casual warming effect, or the absentminded self massage of a scar would have long ago canceled the disturbance field effect. Nonspecific or too many simultaneous interventions lead to a therapeutically meaningless “grey noise”. If I lean on a pillar, I never stimulate the inner branch of the base meridians. A stone in your shoe does not damage internal organs connected through the foot reflex zones at that position. During my first experiments as a neural therapist a patient asked me to produce wheals on all of about three hundred shrapnel scars in a single session. The only result of the procedure was a painfully inflamed thumb saddle joint on my part. Today I am sure: fewer specific interventions are more promising than a variety of simultaneous impulses(2).
The Problem of Disturbance Field Diagnostics
The discovery and therapeutic proof of disturbance fields always requires a lot of reflection and time. An exact anamnesis of the chronological references, a thorough examination and knowledge of the phenomena connected with the disturbance field effect, are indispensable (see [descriptions] below). in order to determine at which of several places I begin the therapy, muscle function tests and devices for measuring changes on the body surface perhaps help as decision-making assistance. Muscle coordination examinations show exclusively whether contact on a body position does or does not deflect the attention from the muscle coordination of the patients. Functional overloading, contusion or disturbance field, the result is always the same coordination deficit. A muscle test cannot prove that a disturbance field is present. The only proof is a successful treatment.
The apparatus methods known to me allow even less evidence. For years John Upledger investigated the Kirlian field. His result: In the Kirlian field you can constantly observe many changes. Specific pathologies or even a therapy recommendation cannot be deduced from it(3). Selective skin resistance measurements, etc. are similarly pointless. This becomes clear in view of the difficulties that already exist in the derivation and interpretation of ECGs. The object of this long investigated, relatively simple measurement is the electrophysiology of the myocardium with clear anatomical and physiological correlates. Already with the EEG it becomes more difficult. To make an objective statement over the body surface about possible disturbance fields with unknown patho-mechanisms, will be a useless hope for a long time. Up to now, the perception ability of our body and our own considerations still beat every machine.
Apparatus methods do not make disturbance field diagnostics possible.
The Disturbance Field and Its Phenomena
There is no chronic disease that inevitably occurs. Every chronically burdened body part (scars, local inflammations, storage of foreign bodies, etc.) can become a disturbance field. The patho-mechanism is not known. Persistent disturbances of the whole regulation irritate predisposed organs and function systems. The self-regulation collapses and the illness follows. Therefore, a disturbance field can work together as a triggering factor for every chronic illness. This evaluation complicates the animal experiment proof from Speranski that the disturbance field conditioned illness can become “autonomous”(5). The reason to search [for a disturbance field] is the failure of otherwise successful therapies. Disturbance fields seldom show a clear self-symptomatology. According to Hoff’s Rule(*) the body immediately counter-regulates dangerous changes. Long-term small stimuli can persistently irritate under the consciousness and counter-regulation margin. More often than the large operation scars, the drainage access scar beside it is a disturbance field. This is specifically why smaller, persistent complaints 6 to 12 months before the first occurrence of the actual symptoms (odontalgia before a root canal treatment, etc.) interest us. It is pointless to “clear” scars that resulted after the first occurrence of the current symptomatology.
Therapy resistant complaints can be the reason for a disturbance field search.
Disturbance Field Phenomena in Overview
- The Second Phenomenon
After injection of a Neural Therapeutic into the disturbance field, all the triggered distant disturbances disappear completely in the same second. For methods without local anesthetics the following somewhat weakened criteria are also valid:
-
- The tooth-jaw area must be pain free from 4 to 8 hours, other areas at least 20 hours
- The therapy effect must be reproducible and every time stop longer
- Everyone must be able to reproduce the phenomenon with Neural Therapy
- Reactions Phenomenon – The Clearest Disturbance Field Indication
A local treatment regularly triggers an increase of the specific complaints no matter what kind – do not mistake with unspecific complaints after a treatment.
- Retrograde Phenomenon (According to Hopfer)
A local treatment unexpectedly triggers complaints in the causal disturbance field.
- Late Phenomenon
The same is valid for this as for the Second Phenomenon; for inflammation, insertion tendinitis, etc. the success sets in somewhat delayed.
- Vegetative and Emotional Reactions (According to Hopfer)
They can be a disturbance field indication, however do not have to be: At first euphoria; compulsory wine without grief [but] with huge crocodile tears; flush, cranial “turning bright scarlet” with abrupt reddening of the collarbone; extreme fatigue after treatment.
Disturbance Field or Rigidity
Rigid regulation can block a successful disturbance field therapy.
Local disturbance fields and global/regional regulation rigidity cause both chronic and therapy resistant complaints. Normal self-regulation is restricted both times. Regulation rigidity originates from, among other things, the intake of medications that inhibit regulation (e.g. no fever with infection, because immediately ASA [aspirin] was always taken early), through persistent distress, faulty nutrition, trauma and many others. Examination possibilities are the Kibler-Fold [skin folding test] or the scratch test on the back (see Fig. 1). Distortion, persistent fading of the skin or flea-bite bleeding (petechia) refer to a chronic burden or rigidity. Glass cupping massage(6), athletics, healing fasts, fever therapies, etc., dissolve rigidity and slowly improve the symptoms. The effect of the disturbance field treatment occurs much more quickly. The disturbance field treatment can remain ineffective if at the same time a regulative rigidity is present. Only after treatment of the rigidity is the disturbance field therapy effective. Sometimes the body compensates the disturbance field burden after reversal of the rigidity and becomes symptom free without local treatment.
 Fig. 1: Patients with healthy reddening reactions
Fig. 1: Patients with healthy reddening reactions
according to the scratch test on the back.
Disturbance fields are just as varied in their genesis as in their symptomatology. One factor seldom leads to a disturbance field reaction. Many scar disturbance fields are primarily unobtrusive. If we treat a scar manually with a simple technique [like] Ortho-Bionomy, we frequently observe strong emotional reactions. For treatment we put our fingertips onto a scar and mobilize them successively and clearly separated in different directions (see Fig. 2). In each case the most pleasant directions are held longer for some breaths. Nevertheless, if strong internal unrest, signs of vegetative stress or clear emotions occur, still more attention is offered. Memories and triggers for memories are stored in the connective tissue. With scar treatment, the whole situational context of the scar genesis can come out again. This must be therapeutically counterbalanced.
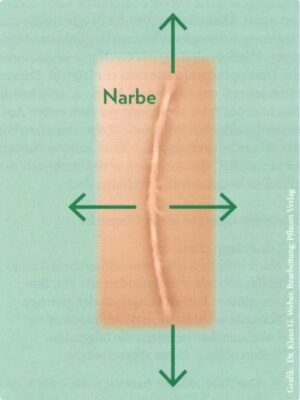 Fig. 2: Scar mobilization [Narbe = Scars]
Fig. 2: Scar mobilization [Narbe = Scars]
In addition to physical disturbance field effects, we take into consideration the following effects of somatopsychic burdens in a scar or an organ. You can explain physical disturbance fields with the analogy of a computer. In the electro-physiology of the body, much is regulated through changes of the electrical potentials. Disturbance fields are zones that change the regulated information transmissions, as if there were leakage currents or as if absolutely pointless impulses were emitted, which confuse the body. Interrupting the current supply with a program crash remains as the final solution. Neural therapy causes exactly that with the membrane blockade.
For memories in the connective tissue that burden the stimulus process as conditioned reflexes, trauma-therapeutic help is needed for our patients. Smaller, socially insignificant traumatizations, which were defined as normal situations in the surroundings, were also suppressed into the subconscious like menacing traumatizations, which could only be managed through repression or at least become tolerable.
Traumatic experiences can be stored in the connective tissue.
Success with clarification of possible “trauma disturbance fields” is promised by the “Ciny Time Zone” – a technique according to Odile Ciny, the lifelong partner of the founder of Ortho Bionomy(**), Arthur Pauls(7). With our patients we mark some of their prominent life situations into a life-circle or a life-line, e.g. a school change, start of a career, deaths, beginning of partnerships, children, retirement.
Afterwards, we relatively quickly trace the whole life process from today back to conception. Then the patient can follow the life circle with a finger on the drawing. With involuntary pausing of the patients – even in unexpected, seemingly harmless occurrences and times – or an internal resonance of the therapist, we mark these periods of life and if necessary consider them more exactly later. This technique opens the memory of an earlier traumatization that can be better integrated today and the stress processing and body coordination can be less burdened in the future.
The perinatal phase occupies a particular importance. Even with a fundamentally normal process, the transformation processes of childbirth lead to various life-stamping danger and stress coping mechanisms. If unpleasant accompanying circumstances turn out for mother, family and child, the prerequisite for the genesis of some energetic-emotional disturbance field events is quickly given.
With this, I wish you the pleasure that differentiates the terms focus illness, rigidity, and physical or energetic-emotional disturbance fields, and that carefully targeted transforms your therapy concepts.

An Exclusive Translated Article for P2P Supporters
From the Monthly Pubications of P2P
Published June 2020
From an article in Naturheilpraxis, Volume 72, June 2019
Machine Translation by SYSTRAN, Lernout & Hauspie, LogoMedia & Promt
Translation & redaction by: Carolyn L. Winsor, P2P Consulting
© Copyright 2019, Dr. med. Klaus G. Weber, Rottenburg, Germany

Footnotes:
(*) Medical Definition of van’t Hoff’s law (1874).
A statement in physical chemistry: the effect of a change in temperature on a system in equilibrium is to shift the equilibrium in the direction that acts to nullify the temperature change. According to van’t Hoff’s law, an increase in temperature will cause an increase in the rate of an endothermic reaction
(**) “What is Ortho-Bionomy?
Ortho-Bionomy is a gentle form of bodywork that has evolved into a unique, complete system of natural healing based on non-force handling of the body’s tension. This safe, natural method ranges from gentle bodywork to the esoteric energy techniques used by advanced practitioners.
The benefits of Ortho-Bionomy are achieved through the body’s own self-corrective reflexes. As the reflexes are monitored by the practitioner, old memory patterns in the body receive new information and are replaced by healthy patterns.
Ortho-Bionomy was developed in 1976 by Arthur Lincoln Pauls, a Canadian osteopath and martial arts instructor.”
Literature
- Weber K., Wiese M.: Weiche manuelle Techniken der OrthoBionomy, 2. Auflage, Sonntag Verlag, Stuttgart 2005
- Weber K.: Neuraltherapie in der Praxis, 2. Auflage, Sonntag Verlag, Stuttgart 2004
- Upledger J.: Im Dialog mit der Zelle – Cell Talk, Haug Verlag, Stuttgart 2006
- Weber K., Wiese M.: Kraniosakrale Therapie, Ressourcenorientierte Behandlungskonzepte, Springer Verlag, Heidelberg 2003
- Speranski A. D.: Grundlagen der Theorie der Medizin, Saenger Verlag, Berlin 1950
- Wiese M., Weber K.: Dynamische und energetische Techniken, Sonntag Verlag, Stuttgart 2006
- Wiese M., Weber K.: Frau sein – genussvollleben ohne Schmerz, Pflaum Verlag, München 2018
")
