
The Chronology of a Mistake,
Part 1
Despite untiring educational work the AIDS myth persistently lasts and through glamorous AIDS galas, money is still collected for the pharmaceutical industry. The general practitioner Juliane Sacher describes here the results of her studies that exposed the official theory as a delusion and yet her results were swept under the table, even though the studies were encouraged and financed by the [German] federal government.
I read about AIDS (Acquired Immune Deficiency Syndrome) for the first time in 1983 in one of the many medical journals. The illness had just been renamed from GRID (= Gay Related Immune Deficiency Syndrome).
It was supposed to be a new illness that spreads among homosexual men and that very quickly leads to death. The search for a new virus was mentioned. They claimed that the illnesses could not be explained differently.
It surprised me that the first five AIDS patients in the USA, from whom the disease was formulated, did not know each other. Thus at first there was no clue for a sexually transmissible illness, but rather for me the question of lifestyle arose.
What was there in common with homosexuals that could be responsible for the disease process?
Peculiar Blood Values
Since I also worked as an occupational health specialist with the German airline Lufthansa since 1975, I had an overview of a large number of blood test results with homosexuals. (Actually a series of the first AIDS patients in Germany were employed by Lufthansa.) Already in the 1970’s I had noticed that an extremely low total leucocyte count frequently occurred in the male flight personnel. I held professional stress and the frequent time-lags responsible for it. Later I heard that it was already known in the 1970’s that frequent passive anal sex has immune suppressive effects. They were of the opinion that the immune system of the receptive partner must grapple with the sperm as a foreign protein every time which can lead to a reduction of the leucocytes. (Continuing immunological examinations of the leucocytes or rather the lymphocyte differentiation were only carried out later in the 1980’s. It was only possible to quantitatively measure the sub-groups of lymphocytes, for example different T-cells, after the monoclonal antibodies were discovered.)
Moreover it was well known that higher contamination was produced among homosexuals with known sexually transmissible diseases, such as Syphilis and Herpes illnesses. Above all the Herpes virus played a large role in all Cytomegalovirus (CMV). Much was reported about that in the 1970’s. In particular, they suspected that the Cytomegalovirus was a cause for Kaposi Sarcoma (malignant vascular tumor under the skin).
Then I heard about the so called promiscuous homosexuals with many different partners per evening, and it was quickly clear to me that a man cannot accomplish the above mentioned number of sexual contacts without sexually stimulative drugs.
Gallo’s Virus Myth
On April 23, 1983 Dr. Robert Gallo announced in a press conference that he had discovered a new virus – HTLVIII, later called HIV – which would destroy the T4 cells and thus was responsible for the AIDS illness. In the history of medicine there has never before been a case where a researcher publicly announced his results before he had published his work about it in a scientific journal.
Already on the same day – as was later established – Gallo had submitted everything for future HIV Tests to the Patent Office. A continuous T4 cell drop had been noticeable with AIDS patients. For test possibilities, they defined the disease AIDS: Either a PCP (= Pneuymocystis carinii Pneumonia, a special lung inflammation) or the previously mentioned Kaposi Sarcoma (KS – a special tumor of the skin), or both together plus a positive HIV test.
Illogical Connections
On the basis of that test, the groups of drug addicts and of hemophiliacs were quite quickly added to the risk group along with homosexuals. There was a publication at the time about the hemophiliac patients, which represented a well documented group because of their illness. The patients were affected by over 80%, while the investigation of the blood donors showed that they were affected only to 0.01%. I immediately noticed the discrepancy of the percentage distribution.
All facts known to me at that time collected together were sufficient for me as an explanation for the individual cases of AIDS. I did not need a new virus to explain the illnesses to me. From the official numbers I could not recognize an epidemic-like propagation of AIDS.
However of course I also had to believe that he had discovered a new virus, since I simply could not say ‘this is not correct’. At that point in time I did not have sufficient understanding of how one recognizes a new virus and how it is isolated. I only had more experience with that at the end of the 1980’s and beginning of the 1990’s. But more about that later – how did it continue chronologically?
In Frankfurt University hospital in the mid-1980’s a small working group of physicians was formed who were interested in the AIDS illness. The working group was led by Prof. Eilke Helm. In the first two years between four and five registered doctors in private practice took part. For me there was one crucial question that nobody could answer at the time.
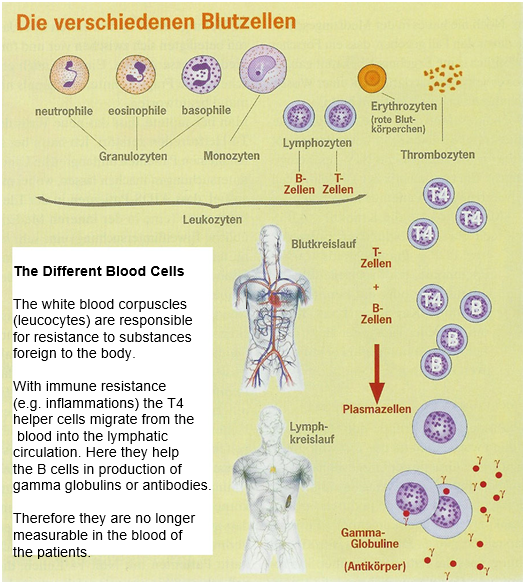
It was stated that the new virus destroys the T4 helper cells. I did extensive laboratory tests with all my patients but what stood out for me was that AIDS patients in electrophoresis (a standard protein examination in internal medicine) had a very high, in some cases extreme number of gamma globulins (also called immune globulins or immune antibodies).
Now I still remembered the little bit that I had learned about immunology for my 1972 state examination. At that time they still knew very little about the immune system. However I remembered why the T4 cells are called helper cells – because they help the B cells to produce plasma cells, and then the gamma globulins (immune globulins or immune antibodies). How could it be that just the patients who have a loss of T4 helper cells (and I had patients with zero T4 cells who were fully able to work!) have such extremely high gamma globulins. I have never seen as high with any disease, namely more than 35-40, even 45 percent, instead of the normal 18 percent?
Actually they already would have had to find out, at that time, what only appeared in experiments many years later: That the T4 cells were not destroyed, but rather that they had migrated out of the blood and are therefore no longer measurable in the blood.
New Explanations
However the first research on this subject was only carried out at the end of the 1980’s and was published at the beginning of the 1990’s. They found out that there is not just one kind of T4 cells, but two kinds, the Th1 and the Th2 cells. They also found out that HIV/AIDS patients have a shift in the balance of Th1/Th2 cells, namely in the direction of Th2 – that means that they have a lack of Th1 and the Th2 even increases. However, these Th2 cells migrate out of the blood to where they can carry out their tasks, namely into the lymph vessels and into the lymph nodes for assistance to the B cells with production of the gamma globulins.
With this knowledge the mystery is solved. They did not need a new virus to explain the T4 cell reduction. As now noted they were not destroyed either, but rather only migrated from the blood into the lymphatic tissue. This then also explained the lymph node swelling typical with HIV/AIDS patients. In this way chronic, difficult to stop inflammations subside.
Now it also became clear why the official “Combo Therapy” [multidrug therapy] (that has a cytostatic effect) often – not always – results that the T4 cells increase in the blood and the lymph node swellings decrease. The “Combo Therapy” suppresses the inflammation processes in the periphery; the T4 cells again migrate back into the blood and again become measurable.
The newest work in recent years also proves that these T4 cells from the blood are in no way a question of newly produced T4 cells. The proof that it is a matter of old T4 cells which could not have been destroyed has been published in recent years. Why do they nevertheless stick to the virus theory? To this day nobody can yet show how HIV destroys the T4 cells.
Why Africa?
It could already be read in all the media, from the very beginning through the middle of the 1980’s that AIDS quite certainly came from Africa. That surprised me because I heard only about cases from the USA and then slowly increasing a few cases in Germany and Europe. But I still had not heard of a case from Africa.
Then in 1985 researchers went to Africa to search for affected persons there.
But very quickly there was a problem in finding these patients, because:
- They could not find patients with PCP lung inflammation
- Kaposi was already there endemically for centuries and the African doctors did not want to get involved with a new disease, and
- There was no money to carry out the HIV tests in Africa.
The African doctors asked them to find a possibility with which they could recognize the supposed AIDS patients. As a result in 1986 a new AIDS definition was determined by the World Health Organization (WHO) for Africa, which in all other respects applies to all developing countries: You can say without a test, but only after an examination, that someone has AIDS if two main criteria and one secondary criterion are met. Specifically the diagnosis of AIDS is not to be placed with cancer, severe malnutrition, Kaposi Sarcoma or Cryptococcal meningitis (Quoted from Quinn et al., AIDS in Africa: An epidemiological paradigm, Science, 21.11.1986).
For adults:
Main criteria: more than 10 percent decrease in weight, more than 1 month of diarrhea, more than 1 month of fever.
Secondary criterion: Cough more than 1 month, generalize itching, fungus infection mouth or neck, generalized chronic Herpes, generalized lymph node swelling.
For children:
Main criteria: more than 10 percent decrease in weight or slow growth, more than 1 month of diarrhea, more than 1 month of fever.
Secondary criterion: generalized lymph node swelling, repeated common infections, fungus in mouth and throat, continuous cough, generalized dermatitis, assured HIV infection of the mother.
You can easily imagine which persons are now designated on the basis of these criteria – without a blood test – as AIDS patients.
From old comes new . . .
In 1993 an “Alternative World AIDS Congress” took place in Amsterdam. There the African doctors told me they knew that with AIDS patients in Africa it was probably more a question of the old diseases, especially malaria and tuberculosis. However, because they get more money from WHO for an AIDS patient than for a malaria or tuberculosis patient, they are more inclined to designate the patients as AIDS patients . . .
The study group of Prof. Eleni Papdopulos-Eleopulos and Prof. Val Turner from Perth, Australia dealt with the HIV test since the 1980’s. They could show that the HIV test is positive with the mentioned illnesses and also in many other cases!(1)
In 1993 Christine Johnson wrote in the English AIDS-critical journal Continuum about numerous scientific papers in which more than 60 different disease states and factors are reported to react positively to the HIV test.
Already six papers with positive test results after flu vaccination, one paper after tetanus vaccination, six papers in connection with acute viral infections, five papers in connection with syphilis, , five papers after kidney transplantations, eight papers in connection with alcohol hepatitis, five papers in connection with multiple pregnancies, etc.
German study does not fit
In order to create a picture of the infection of the alleged virus, the German Federal Government decided to carry out a study in the prisons.
They knew that daily over 20,000 drug addicts serve a sentence, they are often HIV positive, that in prison needle exchange and sexual intercourse take place, and they thought to obtain a measure of the infection danger. The study would run over ten years.
They began it in 1987. All prisoners were tested, all came, and all were dismissed. After two and a half years the study was broken off, because nobody – not one single person – had been infected. Strangely this was not rung like a great bell – it did not fit into the concept.
In the same year of 1987 a study with the same goal was also begun in California. There 442 so called discordant couples (one ♀/♂ HIV positive and one ♀/♂ HIV negative) were attended for over ten years. The partners had both protected and unprotected sexual intercourse.
The results were published in the American Journal of Epidemiology in 1997: No transmission occurred. (Nancy S. Padian, Stephen C. Shiboslei among others in: Am. J. of Epid., University of California, San Francisco, 1997, No. 146, P. 350-357).
Here I would like to mention another two further papers:
A discussion contribution from the Austrian gynecologist Dr. Christian Fiala, written for the closed internet discussion between members of the AIDS Advisory Commission set up by the South African President Thabo Mbeki before the AIDS congress in South Africa: “Epidemiological proofs against the heterosexual transmission of HIV and against prevention campaigns”.
South African President
Thabo Mbeki is committed
to the battle against AIDS
Also from the 2002 published paper of David Gisselquist PhD, Richard Rothenberg MD MPH, John Potterat BA and Ernest Drucker PhD with the title “HIV infections in sub-Saharan Africa not explained by sexual or vertical transmission”, comes out clearly that there are no indications of a sexually infecting disease.
Alternative theories
Now they will ask, okay, so what is it then? You can answer this question yourself, if you have read the book by Dr. Heinrich Kremer. He has meticulously investigated the entire literature of the medical, biological, biochemical, molecular-biological and evolution-biological research and summarized the facts and his findings in the book “Die stille Revolution der Krebs und AIDS-Medizin” [The Quiet Revolution of Cancer and AIDS Medicine – not yet available in English, CLWS]. The miraculous thing is that from these findings the genesis of cancer diseases can also be understood, and from this new and encouraging treatments arise.(2) Every physician should read this book, and also every layman who wants to be treated effectively and as innocuously as possible.
Now what happened at the end of the 1980’s: The HIV Model of the [German] federal government which began in 1987 was carried out in the Georg-Speyer-Hauses in Frankfurt. The leader of the George Speyer House at that time was Prof. Helga Rübsamen-Waigmann who allegedly was the first in Germany to isolate the virus. (More details on this subject in the book “HIV Myth”.) The leader of the HIV Models was Prof. Hans Brede.
The HIV Model was suitable for the recording of patients and for verification of the effectiveness of the new therapy with Azidothymidine (AZT/ZDV = Zidovudine = Retrovir).The Frankfurt area was selected because most AIDS patients lived here (besides Berlin). 95 per cent of the physicians participating with their patients treated those patients with AZT, which was introduced into the USA in 1986 and into Germany starting in 1987.
At that time I had the second biggest (or biggest practice – Berlin doctors and I have never accurately compared) with HIV/AIDS patients in Germany. All my patients were accepted into the HIV Model.
One year after beginning the study the results were announced in a prepublication. It was judged on the basis of the T4 cell drops per year. The T4 cell drop was interpreted respectively as the measure for the seriousness or advancement of the disease. Even today in the USA, among many other criteria, a T4 cell drop under a value of 200 is the absolute criterion for the designation of AIDS.

Patients treated with AZT had a 70 percent drop. The “alternatively” treated patients, which 80-90 percent of my patients were, had only a 7.5 percent drop! Except for myself, only one other physician in Frankfurt treated some patients alternatively, and indeed very successful with homeopathy.
Here it must be said that there was a small group of patients who were HIV positive, but hardly changed blood values and had no complaints, while most other patients were in full blown AIDS, and thus exhibited the defined symptoms.
Financing was assured for the AIDS Model from 1987 on for three years, which in 1990 was assured by the [German] federal government for six further years until 1996, as Prof. Brede proudly and happily reported to me in 1990. In the first week of January 1994 the participants of the HIV Models learned without detailed explanation of the end of the Model Project as of December 31, 1993.
No further results were published from it, and as was later established, all data vanished. If you ask about this today, nobody knows anymore about this federal government assigned and financed study. Also, no one wants to know either in the Bundestag [Lower House of the German Parliament] or the Federal Health Office, about the fact that there are still different treatment approaches than AZT, although the successful treatment of my patients in contrast to the AZT treated patients was proven quite clearly.
By request and reference I communicated my treatment strategy, but no one knows Mrs. Dr. Sacher! Even Dr. Ulrich Marcus claims not to know me although I know him personally. In 1993 at Humboldt University in Berlin he sat beside me on the podium during the premiere of the film “AIDS-Rebellen” [AIDS Rebel]. Among other things this documentary film was co-financed by five states of the German Federal Republic and at that time got the title of “particularly valuable”. That no one in the Bundestag wants to know me is quite astounding, because in 1987 I was invited as an expert by the Bundestag for the AIDS coordinating meeting (more about this is within the extensive minutes) and had mentioned there my view of another therapy.
Protocol [Minutes] of the preparatory meeting of the federal
board of directors and the scientific advisory board with experts.
The next January, 1998 the President inquired by mail with me whether I could send my therapy pattern. In an over 20 page letter I sent my view of the disease and my therapy pattern with a bill for my time involved therein. There was no further correspondence with the President except that he complained in a letter about the fact that I wrote a bill for my work.
In Part 2, Dr. Sacher describes her therapy Part 2
In Part 3, Dr. Sacher describes how alternative therapies can help, Part 3
In Hops and Cocoa against Cancer and Allergies (2010) follow this link
 An confidential article for Members
An confidential article for Members
From THE BRIDGE Newsletter of OIRF
Published February 15, 2007
From an article in raum&zeit, Volume 24, Number 141, May/June 2006
Machine Translation by SYSTRAN, Lernout & Hauspie, LogoMedia & Promt
Translation & redaction by: Carolyn L. Winsor, OIRF
© Copyright 2006, Dr. Juliane Sacher, Frankfurt, Germany

Literature
- Kremer, Heinrich: “Die stille Revolution von Krebs- und AIDS-Medizin”, Ehlers Verlag
- Leitner, Michael: “Mythos HIV”, videel, Niebüll, 2001
Footnotes
- Papadopulos-Eleopulos E.: “Reappraisal of AIDS – Is the oxydation induced by risk factors the primary cause?”, Med. Hypo., 1988, Nr. 25, S. 151 und Papadopulos-Eleopulos E., Turner V, and Papadimitrou J.: “Is a positive Western blot proof of HIV-Infection?”, Bio Technology, 1993, Nr. 11, S. 696-707.
- siehe auch “Vorsicht AIDS-Medizin: Lebensgefahr!”, raum&zeit Nr. 79; “AIDS – ein von Ärzten forciertes Todes-Syndrom ?”, raum&zeit Nr. 86; “Krebs – des Rätsels Lösung?”, raum&zeit Nr. 94; “Wird manipuliertes Eiweiß-Gemisch als AIDS-Test” verkauft”?”, raum&zeit Nr. 95; “Darwins Irrtum und die Krebsmedizin”, raum&zeit Nr. 99; “Afrika: Die Hintergründe der angeblichen AIDS-Seuche”, raum&zeit Nr. 113; “Die tödlichen Irrtümer der Krebs-/ AIDS-Therapeuten”, raum&zeit Nr. 114; “Die Natur der Krebszelle und die Logik der natürlichen Krebsheilung”, raum&zeit Nr. 116; “Die Perversionen der AIDS-Medizin”, raum&zeit Nr.121
")
