
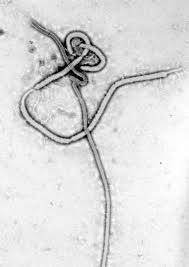
 The Ebola Virus is one type
The Ebola Virus is one type
from the Filoviridae family.
These are usually threadlike,
1,000 to 14,000 nanometers
long and 60 to 80 nanometers
wide in diameter.
After the pandemic is before the pandemic. And thus after Bird Flu, SARS, Swine Flu and EHEC (Enterohaemorrhagic Escherichia coli) we are currently flooded with a new wave of scaremongering by the media: Ebola. Allegedly, in this case it concerns a deadly virus illness against which even our progressive school medicine has still found no remedy. Consequently it says, the epidemic can spread to Germany [or North America] at any time – if we are too negligent. However after the latest swine flu it has been shown that we should look at the facts a little closer before we join the general virus panic.
Therefore how dangerous actually is Ebola?
Please follow this link to see introductory comments to this article. Thank you.
Ebola is the name of a river in Central Africa, on whose shores the first illness cases appeared in 1976. The symptoms began with fever and headaches in almost all cases. In more than 80 percent came pains in the chest and diarrhea. In about 70 percent of the patients the typical bleeding appeared after a few days, more than 60 percent suffered from a painful dry throat, about 60 percent suffered from vomiting, about half from cough and skin rashes or skin flaking off. To this day these are the important leading symptoms of Ebola. The so-called Ebola Virus (EBOV), a threadlike single stranded RNA-virus, is regarded as the cause. Thus morphologically, here it is not distinguishable from the external form of the Marburg Virus (MARV) which can cause the same symptoms as EBOV. Therefore in 1976 they at first suspected a MARV infection, however the corresponding laboratory tests did not strike [did not match]. For this reason the medical teams suspected the existence of a new and so far unknown virus.
Only one out of 10,000 infected becomes ill
The mortality rate of Ebola patients with most outbreaks amounted to more than 50 percent. Therefore the investigating virologist assumed a very great danger from the virus. However at the same time the African population in non-affected areas stood in contradiction to the investigation. The blood tests carried out in 1976 showed that about 5 to 10 percent were antibody positive, and therefore had had contact with the virus without falling ill. Because the antibody values could fall until non-verifiable within weeks, one must assume that the contact with the virus had taken place only recently.
Therefore by no means does contact alone make one sick!

With a renewed outbreak in the Sudan three years later, even 18 percent of the population were tested positive without having fallen ill. The results of the respective investigations varied all together between 2 percent in water proximity and still scarcely 20 percent in forest areas. This could point to the fact that the virus has always circulated in the African population and that the virus alone cannot make you sick at all, but that in addition co-factors are necessary. Beyond this, the outbreaks were usually self limited. The international medical teams on site attributed the end of the outbreaks to their admittedly regular isolation and hygiene measures, however to this day they essentially do nothing more than manage the outbreaks: Every sick person and every contact person is  diligently counted and with the results whole statistics are filled and the medical personnel are very photogenically put into colored “space suits”. However the fact that this ever had a positive influence on the [treatment] course is no more than just a supposition. In 1976 in Zaire there were never more than 10 sick people in the most affected villages. If the virus was really as dangerous as claimed, it would have to have spread explosively at first, and secondly to a large extent the contagion would have to be identical to the illness. However this is not so: Of the approximately one billion people on the African continent possibly up to 200 million came into contact with the virus. Nevertheless the official case figures lie between 5,000 to 6,000 (Sept. 2014). Even if we go with only 50 million Africans with virus contact, therefore with 5 percent contamination, this means that only one in 10,000 infected falls ill. Contact alone with the virus does not by any means make you sick! – thus then is a virus really the cause of the problems?
diligently counted and with the results whole statistics are filled and the medical personnel are very photogenically put into colored “space suits”. However the fact that this ever had a positive influence on the [treatment] course is no more than just a supposition. In 1976 in Zaire there were never more than 10 sick people in the most affected villages. If the virus was really as dangerous as claimed, it would have to have spread explosively at first, and secondly to a large extent the contagion would have to be identical to the illness. However this is not so: Of the approximately one billion people on the African continent possibly up to 200 million came into contact with the virus. Nevertheless the official case figures lie between 5,000 to 6,000 (Sept. 2014). Even if we go with only 50 million Africans with virus contact, therefore with 5 percent contamination, this means that only one in 10,000 infected falls ill. Contact alone with the virus does not by any means make you sick! – thus then is a virus really the cause of the problems?
Actually, quite difficult transmission
Already in 1976 the investigation teams in Central Africa found out that usually a very close and longer sustained contact to a sick person was necessary in order to be sick themselves. It was not sufficient for example to stay overnight in the same room with a patient. In so far as one could understand the transmission pathway, primarily the nursing staff in the medical clinics were infected, and the relatives who looked after their [family] members there. Therefore, the experts presumed contact with the bodily fluids of the sick persons as the greatest risk potential. A transmission, for example, through the air or through door handles (in so far as such are generally existing in the Africa rural areas) is considered as rather unlikely. After nearly 40 years of research a transmission through animals is still also purely supposition.
What else could be the cause of the symptoms?
The leading symptoms of Ebola also appear with numerous other illnesses. Under the circumstances the diagnosing doctor can sometimes too quickly overlook an important cause simply because he was too quick with the diagnosis at hand. The German epidemic authority the Robert-Koch Institute (RKI) writes about alternative diagnoses on their website:
“Malaria is the most important differential diagnosis with regard to tropical diseases in patients with unclear fever. On account of the high lethality of Malaria tropica and its good treatment possibilities, malaria must be excluded or confirmed as soon as possible. [ . . .] Other illnesses from other pathogens like viral hemorrhagic fever (for example Yellow Fever Virus, Lassa Virus, Dengue Virus, representatives of the Hanta Virus, Krim-Kongo Virus) and Hepatitis A should be excluded. Also non-viral illnesses like Typhus abdominalis, plague, rickettsiosis, meningococcal sepsis or other sepsis forms, leptospirosis, hemorrhagic forms of relapsing fevers, bacterial dysentery, perhaps also intoxications must be considered if necessary.”
It is also worth considering a whole series of other viral and bacterial infections as the cause of Ebola symptoms. More or less for the sake of completeness, the RKI also even mentions the possibility of poisoning. If you consider how the CDC (Centers for Disease Control & Prevention) handles the subject, you must highly credit the RKI for their relative diligence with their diagnosis position. Then until recently on the website of the US authority there was at least a remark about the fact that one should also test the patients for malaria. Nevertheless this passage was stricken on 7 August 2014, thus one day before the global WHO warning. Only with that can the statistically grasped number of Ebola patients be artificially raised. The World Health authorities (WHO) even go one step further in the direction of scientific arbitrariness: In their case definition of 9 August 2014 they admit that case definitions can change anytime. Rising and falling case figures in the statistics can thus only be based on the updates of the capture criteria Thus yes, with such health-political measures one can launch an “epidemic” practically any time, or can terminate it if the responsible persons regard this necessary.
Because up to 20 percent of the African population basically reacts test-positive, an Ebola-positive laboratory test by no means indicates that the symptoms were actually caused by EBOV.
Therefore the missing differential diagnosis must lead inevitably to wrong diagnoses and therapies for patients who admittedly show Ebola symptoms however for which quite different causes exist – with possibly life threatening consequences.
Until recently on the website of the US authority was at least the remark about the fact that one should also test the patients for malaria. Nevertheless this passage was stricken on 7 August 2014, thus one day before the global WHO warning.
Confusing antibody values in survivors
It is also remarkable that of the Ebola patients who had completely recovered again from their illness, a certain percentage show no Ebola antibodies. In 1976 the proportion of the recovered without provable antibodies lay between 17 and 22 percent. How was it possible to survive the virus without measurable antibody reaction? Well, at that time the doctors had still heard nothing about the cellular immune system, about which today one knows that it performs the real main work for the defense against injurious particles. At that time there was not yet this explanation possibility. The confusing results could also be based on the unreliability of the laboratory tests. Actually this is picked out as a central theme by the author, but is not further followed up. Understandably: If one questions the laboratory tests, in the end one must also question the virus diagnosis itself.
More on this subject: [in German] A pointed short film article by Michael Leitner can be retrieved at: http://vimeo.com/103391967
Possible alternative causes for Ebola symptoms
Actually, it is self-evident that a doctor considers all possible causes with his diagnostic position. Viruses and bacteria may be part of the top priority but their role in illness or healing events is nevertheless more and more scrutinized. The deficiency of important vital materials like vitamins and minerals or nutrition in general is also part of it. During the current spread of Ebola for example this is of importance in any case since here primarily the poor population is concerned. Also psychic and mental aspects must be considered – psychoneuroimmunology and epigenetics are two of the still very young disciplines which come into these connections. Thirdly, it is the poisonings of all kinds which increasingly play a role, for example with pesticides, additives in food, environmental poisons of all kinds or medication side effects. In 1976 the doctors still did not have so many ideas about vital material deficiencies or environmental poisons, but this can be no real excuse for it if these aspects remained disregarded with the diagnosis position – because both homeopathy as well as Traditional Chinese Medicine have already shown for a very long time how a proper and comprehensive anamneses is carried out.
Nevertheless, no remark can be made about the diagnosis of Ebola, neither in 1976 nor with the current outbreaks in the year 2014. The very first [statistically] grasped Ebola patient fell ill on 27 June 1976 in the south of the central African country of Sudan. It concerned a worker in a cotton factory in the town of Nzara. Further workers fell ill, in addition also some family members and friends. This factory is considered by the experts as the center of the outbreak.
Thus what would have been more obviously opportune than to examine more closely the working conditions of the workers, the chemicals which were used in the processing of the cotton and the cotton itself? Actually there is hardly any [other] useful plant which is sprayed with so many pesticides as a cotton plant. Also the chemicals used in the factory were highly toxic. Thirdly there were numerous rats and other rodents in the factory against which rat poison was possibly used. All these would be possible explanations for the observed illness symptoms. Nothing of this is considered in the publications about the Nzara outbreak. Likewise the side effects of those medications which were routinely given to fever patients were not considered, like for example the anti-malarial Chloroquin, antibiotics, the Yellow Fever vaccination, other vaccinations or also DDT to eliminate insects as potential virus carriers. Interestingly (except with Nzara) with the other outbreaks – at that time like today – just medical clinics are the starting point of the epidemic. And also in Nzara they had a medical clinic at their disposal and the bulk of the first Ebola cases there escalated to heavy courses.
The explanation of the experts: The African clinic personnel were inclined to neglect the simplest hygiene measures like the sterilization of injection needles. Consequently it is unclean needles through which the illness is spread and not the side effects of the medications which were injected through the needles. It is really astonishing, how official medicine strictly hides or holds back the obvious connections.
Thus from 1976 until today the precaution and treatment measures suggested by all the official experts have the potential only to make everything worse. Above all fever patients treated in the medical clinics can in this manner mutate at any time into fatally ill Ebola patients. Also in 2014 the hospitals again stand in the center of the outbreaks. No wonder that the population on site is more and more distrustful in relation to the machinations of the clinic doctors and in relation to the real Ebola diagnosis.
Without a virus no career, fame and honor
Therefore what now is the result of my investigations? First of all it is determined that the Ebola diagnosis is based on an astonishingly negligent approach to the anamnesis. From the start all alternative causes were and are hidden. Beyond this the blind faith in the explanatory power of the laboratory tests is an important requirement, for that time as for the current events. The result is already preprogrammed if exclusively virologists are sent into the outbreak areas. They are in an enormous conflict of interest: If they acknowledge the possibility before themselves that the causes of the illnesses could in truth be of non-viral origin or in relation to the environment, they risk that they themselves could be kicked out of the project in favor of for example the toxicologist. The consequences among others would be the discontinuation of the possibility to publish, a promising career as a virus hunter, the expectation of research money or even a Nobel Prize. Summing up: Without a virus no career, no fame and no honor.
The fairy tale of monocausality
The virologists are the secret rulers of our medical system. As soon as a virologist makes a diagnosis with the help of laboratory tests, all the other medical disciplines must withdraw. One of the bases for the secret seizure of power by the virologists is the dogma of the monocausality of illnesses – the superstition – that one must be able to go back to one single cause for every illness. However that is nonsense. In truth it is always the sum of the stress factors which decide whether the regulation room-to-maneuver of an organism is exceeded. Therefore there are usually several starting points for the treating doctor for successful treatment.
With the workers in the cotton factory in Nzara for example the decontamination ability of their bodies may have been affected by a poor or unilateral nutrition which from contact with the evaporated pesticides of the cotton and the chemicals finally led to simple poisoning reactions. If the patient now receives Chloroquin and a vaccination “as a precaution” in the medical clinic and he is still also deloused with DDT, on the basis of this additional poisoning it would require an especially stable constitution in order not to fall seriously ill with typical Ebola symptoms.
Demand for mixed investigation teams
A fundamental demand must also be that from now on only mixed teams are sent to puzzling outbreaks. These [teams] may consist not only just of virologists, but for example also of toxicologists, environmental medicine, nutritional medicine and hygienists. If I had to decide I would also take experienced homeopaths and TCM experts. The leader of these teams should be a general medical practitioner with interdisciplinary training and orientation, by no means however a virologist.
If one really wants to counteract against the Ebola outbreaks, one must first deny the monocausality and secondly use mixed expert teams. Nevertheless the determining authorities, all at the head of the CDC and the WHO are obviously not ready. What the true reasons and motives behind it may be is however another story again.
 An Exclusive Translated Article for Supporters
An Exclusive Translated Article for Supporters
From THE BRIDGE Newsletter of OIRF
Published November 2014
From an article in raum & zeit, Vol. 33, #192, Nov/Dec 2014
Machine Translation by SYSTRAN, Lernout & Hauspie, LogoMedia & Promt
Translation & redaction by: Carolyn L. Winsor, OIRF
© Copyright 2014, Hans U. P. Tolzin, Herrenberg, Germany

Literature
- Ebola-Symposium in Antwerpen, 1977: Ebola virus Haemorrhagic Fever
- WHO Bull World Health Organ, 1978; 56(2): 247-70
- WHO, Wkly Epidem. Rec.1977, 52, 17-184
- RKI, www.rki.de
- (OC, www.cdc.gov
- ECDC, ecdc.europa.eu
- Wikipedia, Stichwort Ebolafieber, Liste der Ausbrüche mit verlinkten Publikationen
- WHO, Case definition recommendations for Ebola or Marburg Virus Diseases, 9 Aug. 2014
- Fachinformation von Resochin (Wirkstoff Chloroquin)
- impf-report Nr. 104/2014, “Ebola – Virologen allein im Urwald”
- weitere Quellen sind auf Anfrage beim Autor erhältlich
")
