
It is sometimes an obvious answer. Why is it that such a large proportion of my patient base has neurotransmitter imbalances? Depression, anxiety, ADD, mental confusion and bipolar are just a few typical symptoms that are present in over 60% of my cases. The million neuron dollar question is: is this a cause or a sequela? Those of us who are fully engaged in the conceptual framework of the root cause would easily banter about how our current medical thesis is fixated on a reductionist model rather than an understanding the interactions of physiological systems. In fact the famed Albert-Laszio Barbabasi discussed in his systems medicine analysis that “the more we know about the workings of individual genes, banks, or neurons, the less we understand the system as a whole”. So we now move from holism to reductionism and back. The concern with reductionist biology is a mechanistic understanding of genes and proteins that then lead to a misunderstanding of physiological systems and thus the classical ‘symptom chasing’ begins.
It’s an obvious answer. Let’s take a look at both systems when discussing the simplistic concern of depression. It is one of the most serious and costly health problems in our world today and major depression accounts for the second longest number of days lost to disability in the United States. Approximately 15% of adults will experience a severe depressed mood during their lifetime and 15% of these adults will commit suicide. Suicide is the third leading cause of death in youth aged 15-24. More teenagers and young adults die from suicide than from cancer, heart disease, AIDS, birth defects, strokes, pneumonia, influenza and chronic lung disease combined. A Paxil deficiency?
In our paradigm looking at root cause is paramount. Ideas of heavy metals, toxic exposure, pleomorphic imbalances, geopathic disturbances, scar/meridian blockages, latent infections and even past grief/traumas amongst others are thoughts swirling through our mind when faced with these patients. So we treat the cause and can even ‘impression’ the neurotransmitters into the body to kick start the process. Our job is to unhinge the block and allow the body to do what it does naturally. This is an obvious answer.
What if this doesn’t work? Like all of you, I am faced with these refractory to treatment patients. Is it time to look at another model?
The Synaptic Cleft
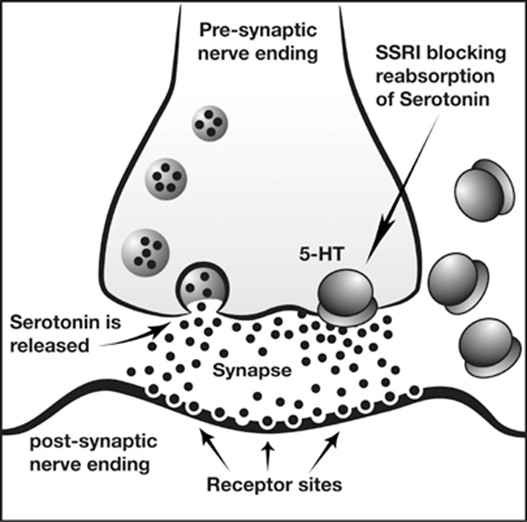
Simply put, tryptophan (amino acid therefore not abundant in vegetarians) requires not just folic acid for conversion to 5HTP but a special type of folic acid called L-5 methyl tetrahydrofolate. This intermediate further requires P5P as well as zinc to convert to the ever ubiquitous serotonin neurotransmitter. Serotonin is considered the first messenger and then travels to the postsynaptic cleft. The second messenger which is often forgotten by most practitioners is inositol. This should also be imbedded into your protocol. It is of absolute importance that I mention to you that almost 80% of the serotonin in the body is not produced in the brain as was once thought, but in the digestive system (hence the term ‘second brain’). The digestive system is the largest receiver and producer of serotonin in the body. This is why the digestive system needs to be treated as well.
Not only should the amount of serotonin be addressed, but also should its breakdown. Monoamine oxidase is responsible for the degradation of serotonin. It seems that curcuminoids and quercetin inactivate this degradation and keep serotonin around longer. The reuptake of serotonin is also modulated by Rhodiaola and green tea. Thus it would be advisable to also include these into your protocol.
It seems like an obvious answer.
With utmost sincerity I advise to look at the root cause. But I preach to the choir. However, with the seemingly opposing view this reductionist model is to not be thrown out. To microanalyze each neuron and its adjacent cofactors is also of vital importance when putting together a protocol. But let me be clear. This is to only slightly augment our protocol. With our every fiber, we must look for the root. Everything else is a side show.
So it does seem like an obvious answer.
In health
Dr. Karim Dhanani
 An Exclusive Article for OIRF Supporters
An Exclusive Article for OIRF Supporters
From THE BRIDGE Newsletter of OIRF
Published May 2014
© Copyright 2014, Karim Dhanani, ND, ON Canada

")
